We aimed to investigate the association between visit-to-visit heart rate variability (VVHRV) and all-cause mortality in patients diagnosed with atrial fibrillation (AF). Previous studies have shown a positive correlation between VVHRV and several adverse outcomes. However, the relationship between VVHRV and the prognosis of AF remains uncertain.
In our study, we aimed to examine the relationship between VVHRV and mortality rates among 3983 participants with AF, who were part of the AFFIRM study (Atrial Fibrillation Follow-Up Investigation of Rhythm Management). We used the standard deviation of heart rate (HRSD) to measure VVHRV and divided the patients into four groups based on quartiles of HRSD (1st, <5.69; 2nd, 5.69–8.00; 3rd, 8.01–11.01; and 4th, ≥11.02). Our primary endpoint was all-cause death, and we estimated the hazard ratios for mortality using the Cox proportional hazard regressions.
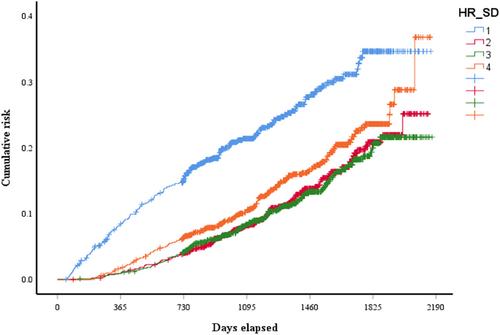
Our analysis included 3983 participants from the AFFIRM study and followed for an average of 3.5 years. During this period, 621 participants died from all causes. In multiple-adjustment models, we found that the lowest and highest quartiles of HRSD independently predicted an increased risk of all-cause mortality compared to the other two quartiles, presenting a U-shaped relationship (1st vs 2nd, hazard ratio = 2.28, 95% CI = 1.63–3.20, p < .01; 1st vs. 3rd, hazard ratio = 2.23, 95% CI = 1.60–3.11, p < .01; 4th vs. 2nd, hazard ratio = 1.82, 95% CI = 1.26–2.61, p < .01; and 4th vs. 3rd, hazard ratio = 1.78, 95% CI = 1.25–2.52, p < .01).
In patients with AF, we found that both lower VVHRV and higher VVHRV increased the risk of all-cause mortality, indicating a U-shaped curve relationship.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
