Mohamed Ahmed Mousa, Sherif Samir El Zahwy, Ahmed Fathy Tamara, Wafed Samir, Mahmoud Ahmed Tantawy
{"title":"外科切开器和经皮闭合器在大口径动脉通路管理中的比较研究。","authors":"Mohamed Ahmed Mousa, Sherif Samir El Zahwy, Ahmed Fathy Tamara, Wafed Samir, Mahmoud Ahmed Tantawy","doi":"10.1186/s42155-023-00395-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Compared to conventional open surgery, minimally invasive catheter-based procedures have less post procedural complications. Transcatheter aortic valve implantation (TAVI) and endovascular aneurysm repair (EVAR) require large bore arterial access. Optimal site management of large bore arterial access is pivotal to reduce the hospital-acquired complications associated with large bore arterial access. We wanted to compare surgical cutdown versus percutaneous closure devices in site management of large bore arterial access.</p><p><strong>Methods: </strong>Participants planned for TAVI or EVAR with large bore arterial access more than 10 French were included, while participants with history of bypass surgery, malignancies, thrombophilia, or sepsis were excluded. A consecutive sample of 100 participants (mean age 74.66 ± 2.65 years, 61% males) was selected, underwent TAVI or EVAR with surgical cutdown (group 1) versus TAVI or EVAR with Proglide™ percutaneous closure device (group 2).</p><p><strong>Results: </strong>The incidence rate of hematoma was significantly lower in group 2 versus group 1 (p = 0.014), the mean procedure time (minutes) and the median hospital stay (days) were significantly higher in group 1 versus group 2 (t(98) = - 2.631, p = 0.01, and U = 2.403, p = 0.018, respectively), and the c-reactive protein pre-procedure and the c-reactive protein post-procedure were significantly lower in group 2 versus group 1 (U = -2.969, p = 0.003, and U = -2.674, p = 0.007, respectively).</p><p><strong>Conclusions: </strong>Our study showed a lower incidence rate of large bore arterial access complications as hematoma, a shorter procedure time, and a shorter hospital stay with percutaneous closure devices compared to surgical cutdown.</p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":null,"pages":null},"PeriodicalIF":1.2000,"publicationDate":"2023-10-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10613603/pdf/","citationCount":"0","resultStr":"{\"title\":\"A comparative study between surgical cut down and percutaneous closure devices in management of large bore arterial access.\",\"authors\":\"Mohamed Ahmed Mousa, Sherif Samir El Zahwy, Ahmed Fathy Tamara, Wafed Samir, Mahmoud Ahmed Tantawy\",\"doi\":\"10.1186/s42155-023-00395-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Compared to conventional open surgery, minimally invasive catheter-based procedures have less post procedural complications. Transcatheter aortic valve implantation (TAVI) and endovascular aneurysm repair (EVAR) require large bore arterial access. Optimal site management of large bore arterial access is pivotal to reduce the hospital-acquired complications associated with large bore arterial access. We wanted to compare surgical cutdown versus percutaneous closure devices in site management of large bore arterial access.</p><p><strong>Methods: </strong>Participants planned for TAVI or EVAR with large bore arterial access more than 10 French were included, while participants with history of bypass surgery, malignancies, thrombophilia, or sepsis were excluded. A consecutive sample of 100 participants (mean age 74.66 ± 2.65 years, 61% males) was selected, underwent TAVI or EVAR with surgical cutdown (group 1) versus TAVI or EVAR with Proglide™ percutaneous closure device (group 2).</p><p><strong>Results: </strong>The incidence rate of hematoma was significantly lower in group 2 versus group 1 (p = 0.014), the mean procedure time (minutes) and the median hospital stay (days) were significantly higher in group 1 versus group 2 (t(98) = - 2.631, p = 0.01, and U = 2.403, p = 0.018, respectively), and the c-reactive protein pre-procedure and the c-reactive protein post-procedure were significantly lower in group 2 versus group 1 (U = -2.969, p = 0.003, and U = -2.674, p = 0.007, respectively).</p><p><strong>Conclusions: </strong>Our study showed a lower incidence rate of large bore arterial access complications as hematoma, a shorter procedure time, and a shorter hospital stay with percutaneous closure devices compared to surgical cutdown.</p>\",\"PeriodicalId\":52351,\"journal\":{\"name\":\"CVIR Endovascular\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2023-10-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10613603/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"CVIR Endovascular\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42155-023-00395-6\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-023-00395-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A comparative study between surgical cut down and percutaneous closure devices in management of large bore arterial access.
Background: Compared to conventional open surgery, minimally invasive catheter-based procedures have less post procedural complications. Transcatheter aortic valve implantation (TAVI) and endovascular aneurysm repair (EVAR) require large bore arterial access. Optimal site management of large bore arterial access is pivotal to reduce the hospital-acquired complications associated with large bore arterial access. We wanted to compare surgical cutdown versus percutaneous closure devices in site management of large bore arterial access.
Methods: Participants planned for TAVI or EVAR with large bore arterial access more than 10 French were included, while participants with history of bypass surgery, malignancies, thrombophilia, or sepsis were excluded. A consecutive sample of 100 participants (mean age 74.66 ± 2.65 years, 61% males) was selected, underwent TAVI or EVAR with surgical cutdown (group 1) versus TAVI or EVAR with Proglide™ percutaneous closure device (group 2).
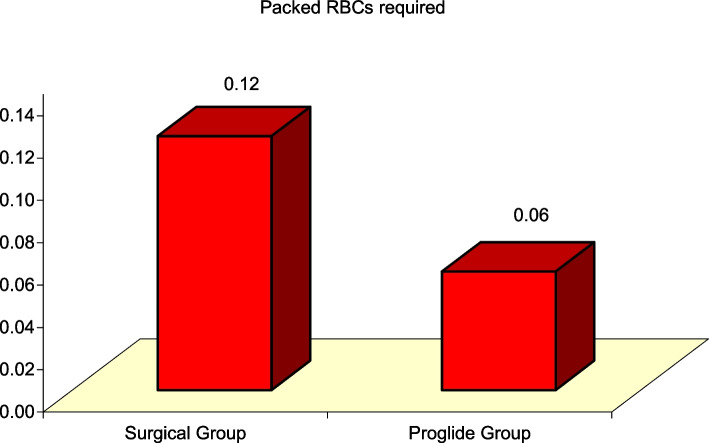
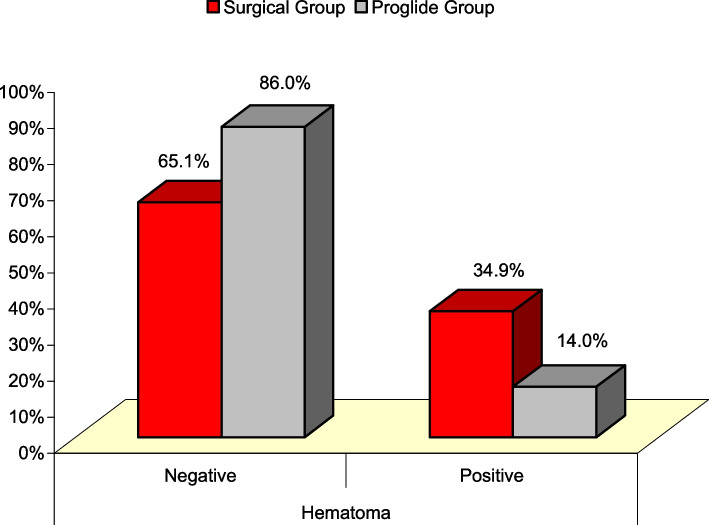
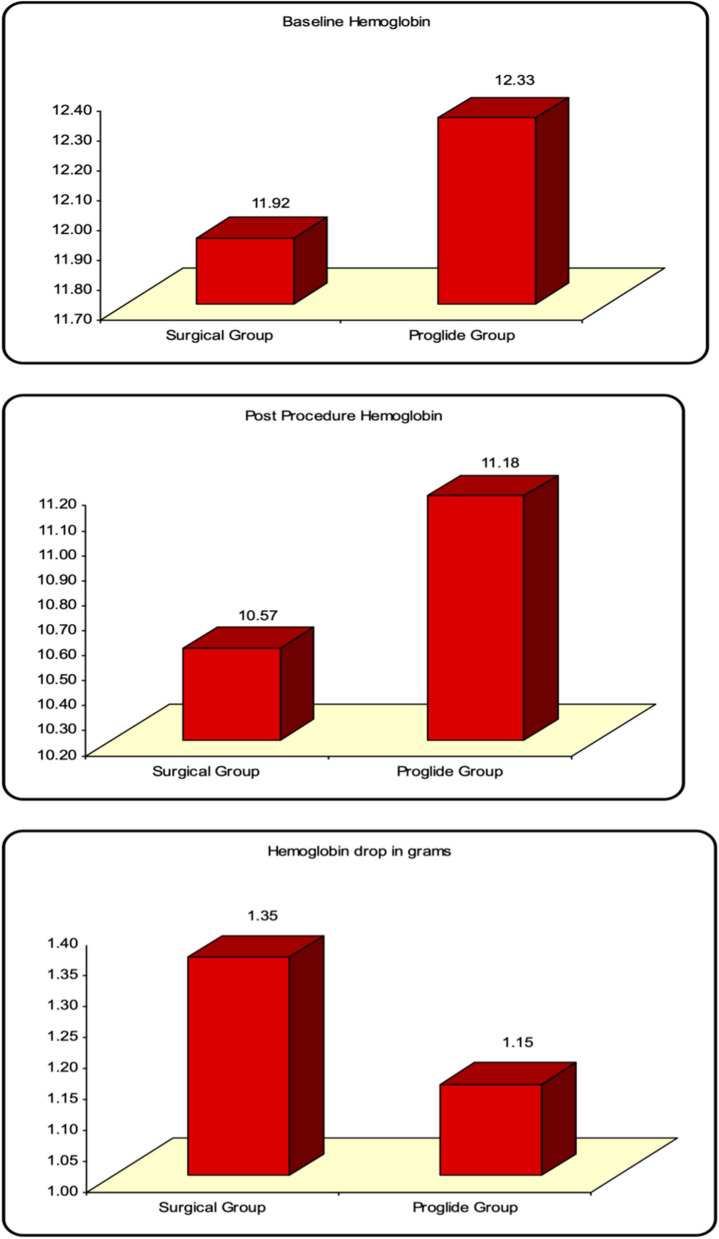
Results: The incidence rate of hematoma was significantly lower in group 2 versus group 1 (p = 0.014), the mean procedure time (minutes) and the median hospital stay (days) were significantly higher in group 1 versus group 2 (t(98) = - 2.631, p = 0.01, and U = 2.403, p = 0.018, respectively), and the c-reactive protein pre-procedure and the c-reactive protein post-procedure were significantly lower in group 2 versus group 1 (U = -2.969, p = 0.003, and U = -2.674, p = 0.007, respectively).
Conclusions: Our study showed a lower incidence rate of large bore arterial access complications as hematoma, a shorter procedure time, and a shorter hospital stay with percutaneous closure devices compared to surgical cutdown.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
