Ease of Intubation with McGrath Videolaryngoscope and Incidence of Adverse Events During Tracheal Intubation in COVID-19 Patients: A Prospective Observational Study.
Faisal Shamim, Muhammad Sohaib, Khalid Samad, Muhammad Faisal Khan, Adil A Manji, Asad Latif
{"title":"Ease of Intubation with McGrath Videolaryngoscope and Incidence of Adverse Events During Tracheal Intubation in COVID-19 Patients: A Prospective Observational Study.","authors":"Faisal Shamim, Muhammad Sohaib, Khalid Samad, Muhammad Faisal Khan, Adil A Manji, Asad Latif","doi":"10.2478/jccm-2023-0020","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Tracheal intubation in critically ill patients remains high-risk despite advances in equipment, technique, and clinical guidelines. Many patients with COVID-19 were in respiratory distress and required intubation that is considered an aerosol-generating procedure (AGP). The transition to videolaryngoscopy as a routine first line option throughout anesthetic and ICU practice has been reported. We evaluated the ease of intubation, success rate, use of accessory maneuvers and adverse outcomes during and 24 hours after intubation with the McGrath videolaryngoscope.</p><p><strong>Methods: </strong>This was a prospective, observational single center study conducted at non-operating room locations that included all adults (>18 years old) with suspected or confirmed COVID-19 infection and were intubated by McGrath videolaryngoscope. The anesthesiologist performed tracheal intubation were requested to fill online data collection form. A co-investigator was responsible to coordinate daily with assigned consultants for COVID intubation and follow up of patients at 24 hours after intubation.</p><p><strong>Results: </strong>A total of 105 patients were included in our study. Patients were predominantly male (n=78; 74.3%), their COVID status was either confirmed (n=97, 92.4%) or suspected (n=8, 7.6%). Most were intubated in the COVID ward (n=59, 56.2%) or COVID ICU (n=23, 21.9%). The overall success rate of intubation with McGrath in the first attempt was 82.9%. The glottic view was either full (n=85, 80.95%), partial (n=16, 15.24%) or none (n=4, 3.81%). During intubation, hypoxemia occurred in 18.1% and hypotension in 16.2% patients. Within 24 hours of intubation, pneumothorax occurred in 1.9%, cardiac arrest and return of spontaneous circulation in 6.7% and mortality in 13.3% of patients.</p><p><strong>Conclusion: </strong>These results illustrate the ease and utility of the McGrath videolaryngoscope for tracheal intubation in COVID-19 patients. Its disposable blade is of significant value in protectin during tracheal intubation.</p>","PeriodicalId":73696,"journal":{"name":"","volume":"9 3","pages":"162-169"},"PeriodicalIF":0.0,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10425925/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jccm-2023-0020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Tracheal intubation in critically ill patients remains high-risk despite advances in equipment, technique, and clinical guidelines. Many patients with COVID-19 were in respiratory distress and required intubation that is considered an aerosol-generating procedure (AGP). The transition to videolaryngoscopy as a routine first line option throughout anesthetic and ICU practice has been reported. We evaluated the ease of intubation, success rate, use of accessory maneuvers and adverse outcomes during and 24 hours after intubation with the McGrath videolaryngoscope.
Methods: This was a prospective, observational single center study conducted at non-operating room locations that included all adults (>18 years old) with suspected or confirmed COVID-19 infection and were intubated by McGrath videolaryngoscope. The anesthesiologist performed tracheal intubation were requested to fill online data collection form. A co-investigator was responsible to coordinate daily with assigned consultants for COVID intubation and follow up of patients at 24 hours after intubation.
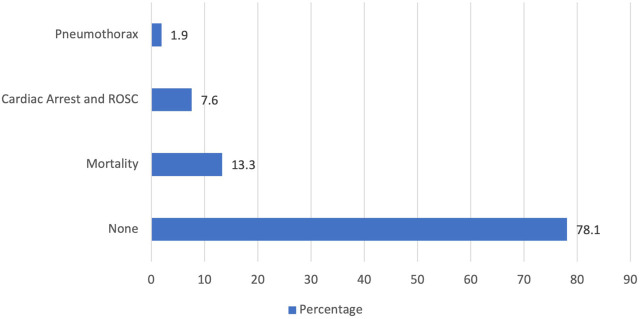
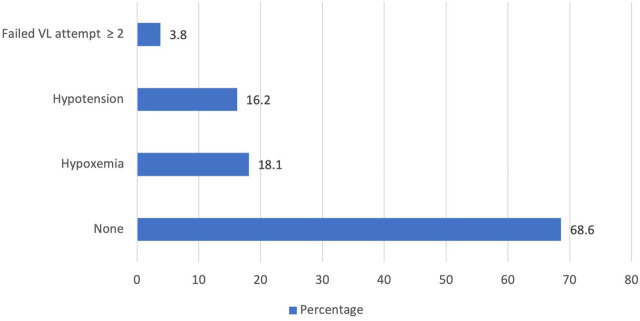
Results: A total of 105 patients were included in our study. Patients were predominantly male (n=78; 74.3%), their COVID status was either confirmed (n=97, 92.4%) or suspected (n=8, 7.6%). Most were intubated in the COVID ward (n=59, 56.2%) or COVID ICU (n=23, 21.9%). The overall success rate of intubation with McGrath in the first attempt was 82.9%. The glottic view was either full (n=85, 80.95%), partial (n=16, 15.24%) or none (n=4, 3.81%). During intubation, hypoxemia occurred in 18.1% and hypotension in 16.2% patients. Within 24 hours of intubation, pneumothorax occurred in 1.9%, cardiac arrest and return of spontaneous circulation in 6.7% and mortality in 13.3% of patients.
Conclusion: These results illustrate the ease and utility of the McGrath videolaryngoscope for tracheal intubation in COVID-19 patients. Its disposable blade is of significant value in protectin during tracheal intubation.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
