James M McMahon, Judith Brasch, Eric Podsiadly, Leilani Torres, Robert Quiles, Evette Ramos, Hugh F Crean, Jessica E Haberer
{"title":"Procurement of patient medical records from multiple health care facilities for public health research: feasibility, challenges, and lessons learned.","authors":"James M McMahon, Judith Brasch, Eric Podsiadly, Leilani Torres, Robert Quiles, Evette Ramos, Hugh F Crean, Jessica E Haberer","doi":"10.1093/jamiaopen/ooad040","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Studies that combine medical record and primary data are typically conducted in a small number of health care facilities (HCFs) covering a limited catchment area; however, depending on the study objectives, validity may be improved by recruiting a more expansive sample of patients receiving care across multiple HCFs. We evaluate the feasibility of a novel protocol to obtain patient medical records from multiple HCFs using a broad representative sampling frame.</p><p><strong>Materials and methods: </strong>In a prospective cohort study on HIV pre-exposure prophylaxis utilization, primary data were collected from a representative sample of community-dwelling participants; voluntary authorization was obtained to access participants' medical records from the HCF at which they were receiving care. Medical record procurement procedures were documented for later analysis.</p><p><strong>Results: </strong>The cohort consisted of 460 participants receiving care from 122 HCFs; 81 participants were lost to follow-up resulting in 379 requests for medical records submitted to HCFs, and a total of 343 medical records were obtained (91% response rate). Less than 20% of the medical records received were in electronic form. On average, the cost of medical record acquisition was $120 USD per medical record.</p><p><strong>Conclusions: </strong>Obtaining medical record data on research participants receiving care across multiple HCFs was feasible, but time-consuming and resulted in appreciable missing data. Researchers combining primary data with medical record data should select a sampling and data collection approach that optimizes study validity while weighing the potential benefits (more representative sample; inclusion of HCF-level predictors) and drawbacks (cost, missing data) of obtaining medical records from multiple HCFs.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"6 2","pages":"ooad040"},"PeriodicalIF":3.4000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/d6/ooad040.PMC10264223.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooad040","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: Studies that combine medical record and primary data are typically conducted in a small number of health care facilities (HCFs) covering a limited catchment area; however, depending on the study objectives, validity may be improved by recruiting a more expansive sample of patients receiving care across multiple HCFs. We evaluate the feasibility of a novel protocol to obtain patient medical records from multiple HCFs using a broad representative sampling frame.
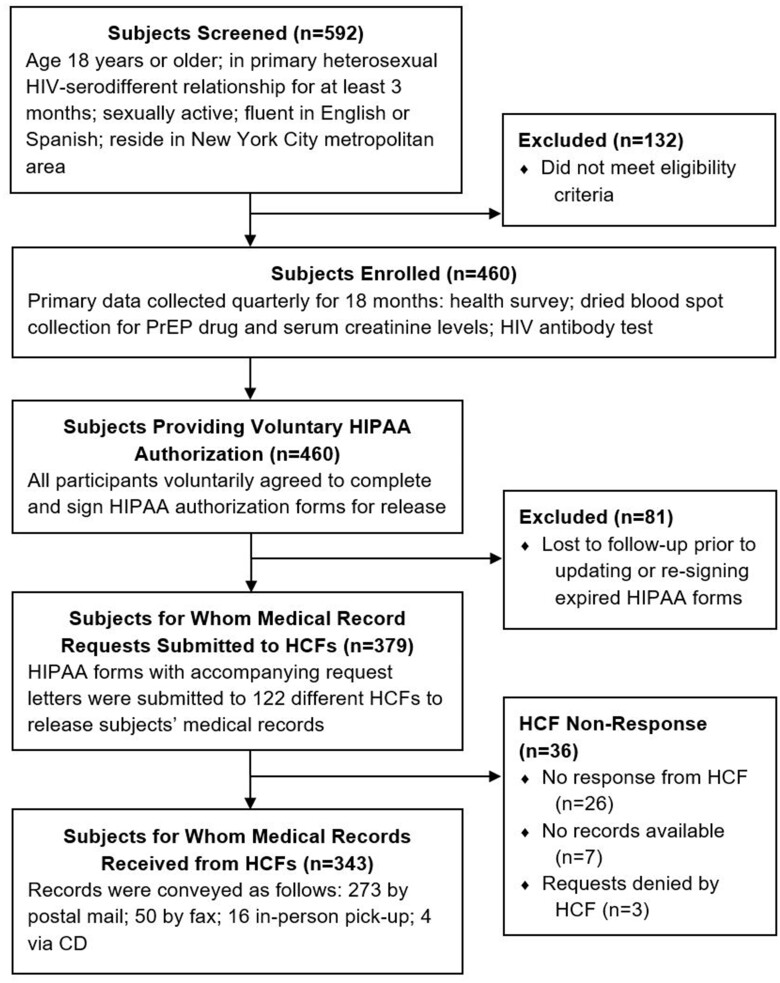
Materials and methods: In a prospective cohort study on HIV pre-exposure prophylaxis utilization, primary data were collected from a representative sample of community-dwelling participants; voluntary authorization was obtained to access participants' medical records from the HCF at which they were receiving care. Medical record procurement procedures were documented for later analysis.
Results: The cohort consisted of 460 participants receiving care from 122 HCFs; 81 participants were lost to follow-up resulting in 379 requests for medical records submitted to HCFs, and a total of 343 medical records were obtained (91% response rate). Less than 20% of the medical records received were in electronic form. On average, the cost of medical record acquisition was $120 USD per medical record.
Conclusions: Obtaining medical record data on research participants receiving care across multiple HCFs was feasible, but time-consuming and resulted in appreciable missing data. Researchers combining primary data with medical record data should select a sampling and data collection approach that optimizes study validity while weighing the potential benefits (more representative sample; inclusion of HCF-level predictors) and drawbacks (cost, missing data) of obtaining medical records from multiple HCFs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
