James J M Loan, Steven Tominey, Kirun Baweja, Julie Woodfield, Thomas J G Chambers, Mark Haley, Simran S Kundu, H Y Josephine Tang, Anthony N Wiggins, Michael T C Poon, Paul M Brennan
{"title":"Prospective, multicentre study of screening, investigation and management of hyponatraemia after subarachnoid haemorrhage in the UK and Ireland.","authors":"James J M Loan, Steven Tominey, Kirun Baweja, Julie Woodfield, Thomas J G Chambers, Mark Haley, Simran S Kundu, H Y Josephine Tang, Anthony N Wiggins, Michael T C Poon, Paul M Brennan","doi":"10.1136/svn-2022-001583","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hyponatraemia often occurs after subarachnoid haemorrhage (SAH). However, its clinical significance and optimal management are uncertain. We audited the screening, investigation and management of hyponatraemia after SAH.</p><p><strong>Methods: </strong>We prospectively identified consecutive patients with spontaneous SAH admitted to neurosurgical units in the United Kingdom or Ireland. We reviewed medical records daily from admission to discharge, 21 days or death and extracted all measurements of serum sodium to identify hyponatraemia (<135 mmol/L). Main outcomes were death/dependency at discharge or 21 days and admission duration >10 days. Associations of hyponatraemia with outcome were assessed using logistic regression with adjustment for predictors of outcome after SAH and admission duration. We assessed hyponatraemia-free survival using multivariable Cox regression.</p><p><strong>Results: </strong>175/407 (43%) patients admitted to 24 neurosurgical units developed hyponatraemia. 5976 serum sodium measurements were made. Serum osmolality, urine osmolality and urine sodium were measured in 30/166 (18%) hyponatraemic patients with complete data. The most frequently target daily fluid intake was >3 L and this did not differ during hyponatraemic or non-hyponatraemic episodes. 26% (n/N=42/164) patients with hyponatraemia received sodium supplementation. 133 (35%) patients were dead or dependent within the study period and 240 (68%) patients had hospital admission for over 10 days. In the multivariable analyses, hyponatraemia was associated with less dependency (adjusted OR (aOR)=0.35 (95% CI 0.17 to 0.69)) but longer admissions (aOR=3.2 (1.8 to 5.7)). World Federation of Neurosurgical Societies grade I-III, modified Fisher 2-4 and posterior circulation aneurysms were associated with greater hazards of hyponatraemia.</p><p><strong>Conclusions: </strong>In this comprehensive multicentre prospective-adjusted analysis of patients with SAH, hyponatraemia was investigated inconsistently and, for most patients, was not associated with changes in management or clinical outcome. This work establishes a basis for the development of evidence-based SAH-specific guidance for targeted screening, investigation and management of high-risk patients to minimise the impact of hyponatraemia on admission duration and to improve consistency of patient care.</p>","PeriodicalId":22021,"journal":{"name":"Stroke and Vascular Neurology","volume":"8 3","pages":"207-216"},"PeriodicalIF":4.9000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10359796/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke and Vascular Neurology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2022-001583","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Hyponatraemia often occurs after subarachnoid haemorrhage (SAH). However, its clinical significance and optimal management are uncertain. We audited the screening, investigation and management of hyponatraemia after SAH.
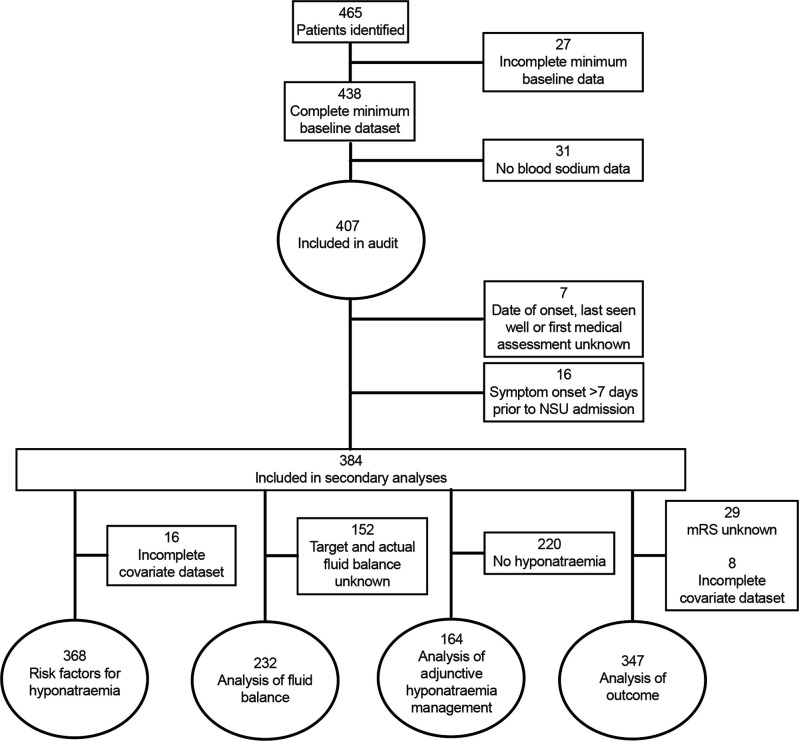
Methods: We prospectively identified consecutive patients with spontaneous SAH admitted to neurosurgical units in the United Kingdom or Ireland. We reviewed medical records daily from admission to discharge, 21 days or death and extracted all measurements of serum sodium to identify hyponatraemia (<135 mmol/L). Main outcomes were death/dependency at discharge or 21 days and admission duration >10 days. Associations of hyponatraemia with outcome were assessed using logistic regression with adjustment for predictors of outcome after SAH and admission duration. We assessed hyponatraemia-free survival using multivariable Cox regression.
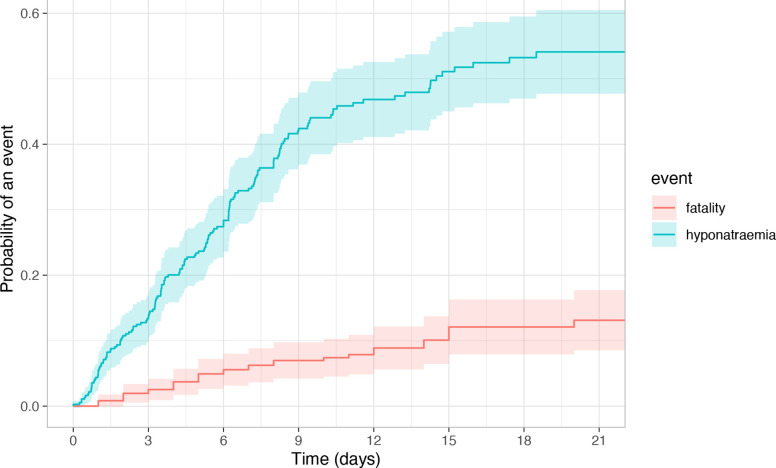
Results: 175/407 (43%) patients admitted to 24 neurosurgical units developed hyponatraemia. 5976 serum sodium measurements were made. Serum osmolality, urine osmolality and urine sodium were measured in 30/166 (18%) hyponatraemic patients with complete data. The most frequently target daily fluid intake was >3 L and this did not differ during hyponatraemic or non-hyponatraemic episodes. 26% (n/N=42/164) patients with hyponatraemia received sodium supplementation. 133 (35%) patients were dead or dependent within the study period and 240 (68%) patients had hospital admission for over 10 days. In the multivariable analyses, hyponatraemia was associated with less dependency (adjusted OR (aOR)=0.35 (95% CI 0.17 to 0.69)) but longer admissions (aOR=3.2 (1.8 to 5.7)). World Federation of Neurosurgical Societies grade I-III, modified Fisher 2-4 and posterior circulation aneurysms were associated with greater hazards of hyponatraemia.
Conclusions: In this comprehensive multicentre prospective-adjusted analysis of patients with SAH, hyponatraemia was investigated inconsistently and, for most patients, was not associated with changes in management or clinical outcome. This work establishes a basis for the development of evidence-based SAH-specific guidance for targeted screening, investigation and management of high-risk patients to minimise the impact of hyponatraemia on admission duration and to improve consistency of patient care.
期刊介绍:
Stroke and Vascular Neurology (SVN) is the official journal of the Chinese Stroke Association. Supported by a team of renowned Editors, and fully Open Access, the journal encourages debate on controversial techniques, issues on health policy and social medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
