Mariana Ortega Perez, Pedro Paulo de Alcantara Pedro, André Marun Lyrio, Felipe Merchan Ferraz Grizzo, Marco Antonio A da Rocha Loures
{"title":"Osteoporosis and fracture risk assessment: improving outcomes in postmenopausal women.","authors":"Mariana Ortega Perez, Pedro Paulo de Alcantara Pedro, André Marun Lyrio, Felipe Merchan Ferraz Grizzo, Marco Antonio A da Rocha Loures","doi":"10.1590/1806-9282.2023S130","DOIUrl":null,"url":null,"abstract":"Osteoporosis is a skeletal disease characterized by impaired bone density, bone mineral density (BMD), and bone strength, resulting in bone fragility and an increased risk of fractures1. A fracture is the worst outcome for patients with osteoporosis, as it increases morbidity and mortality in addition to increasing the risk of new subsequent fractures. The main cause of osteoporosis in women is estrogen deficiency secondary to menopause2,3. Osteoporosis has a high prevalence and a social and financial impact. The prevalence of the diagnosis of osteopenia in postmenopausal women was present in 30–56.5% of the population, and osteoporosis enters the range of 14.7–43.4%4. Osteoporosis can lead to a major impact on public health, such as hospitalizations, surgeries with prostheses, temporary or permanent loss of mobility, and death2,3. Although BMD is a strong predictor of fracture risk, there are patients who may fracture even without presenting osteoporosis in the bone densitometry exam, making it necessary to evaluate risk factors other than bone density. In this context, the FRAX (Fracture Risk Assessment Tool) tool brings together other risk factors for fracture prediction independent of BMD, such as the presence of previous fragility fracture, hip fragility fracture in the parents, current smoking, use of glucocorticoids, rheumatoid arthritis, secondary osteoporosis, and use of three or more units of alcoholic beverage per day1-4. Interestingly, FRAX is an algorithm that analyzes all clinical risk factors together and finally calculates the absolute risk of fracture in 10 years. Patients diagnosed with osteoporosis or those at high risk of fracture by FRAX deserve drug treatment targeting bone mass gain and fracture prevention. Among the drug strategies are anti-resorptive drugs (bisphosphonates and denosumab) and anabolic agents (teriparatide and romosozumab), which must be associated with other measures, such as physical activity, calcium intake, preferably in the diet, and supplementation of vitamin D2. The prevalence of osteoporosis increases with age, with a consequent increase in the number of fractures, either due to worsening of the bone structure, with thinning of the cortical bone, reduction of the trabeculae, and alteration of the bone microarchitecture, or due to the increased risk of falls, reduced lean mass, impairment of proprioception, and decreased visual acuity, among other factors. Osteoporotic fractures are those due to fragility, that is, low impact. Fragility fractures may be asymptomatic, mostly when occurred in the vertebral bodies with wedging, leading to height loss and dorsal hyperkyphosis5. Annually, almost 9 million fractures occur worldwide due to osteoporosis, which corresponds to an osteoporosis-related fracture every 3 s, and of these fractures, 1.6 million are hip fractures. The world estimate is that there are about 500 million people with osteoporosis, predominantly women, with an estimated fracture resulting from osteoporosis occurring in one in three women over 50 years and one in five men in the same age group5. BMD is directly related to fracture risk. The loss of 10% of BMD in the spine is associated with twice the risk of fracture, and the same loss of BMD in the hip leads to an increase in the risk of fracture by two and a half times. A previous fracture increases the risk of a new fracture by 86%, mainly in the subsequent 2 years. Despite the financial cost, morbidity, and mortality associated with osteoporosis, evidence shows that up to 80% of women with fragility fractures are not diagnosed or treated for osteoporosis5.","PeriodicalId":21234,"journal":{"name":"Revista da Associacao Medica Brasileira","volume":"69 suppl 1","pages":"e2023S130"},"PeriodicalIF":1.3000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8e/b1/1806-9282-ramb-69-suppl1-e2023S130.PMC10411691.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista da Associacao Medica Brasileira","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1590/1806-9282.2023S130","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
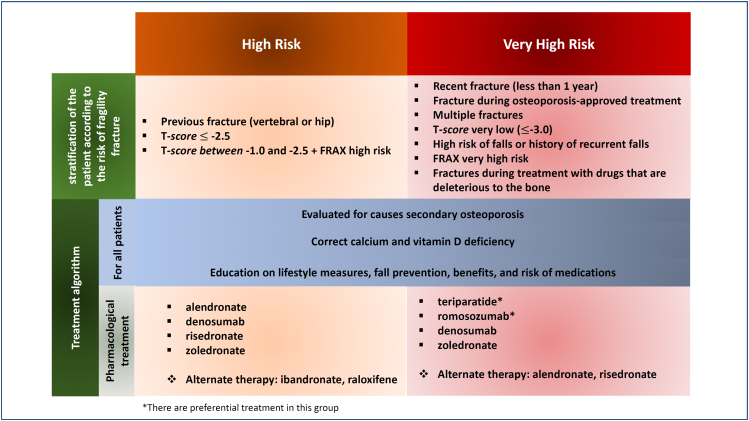
Osteoporosis is a skeletal disease characterized by impaired bone density, bone mineral density (BMD), and bone strength, resulting in bone fragility and an increased risk of fractures1. A fracture is the worst outcome for patients with osteoporosis, as it increases morbidity and mortality in addition to increasing the risk of new subsequent fractures. The main cause of osteoporosis in women is estrogen deficiency secondary to menopause2,3. Osteoporosis has a high prevalence and a social and financial impact. The prevalence of the diagnosis of osteopenia in postmenopausal women was present in 30–56.5% of the population, and osteoporosis enters the range of 14.7–43.4%4. Osteoporosis can lead to a major impact on public health, such as hospitalizations, surgeries with prostheses, temporary or permanent loss of mobility, and death2,3. Although BMD is a strong predictor of fracture risk, there are patients who may fracture even without presenting osteoporosis in the bone densitometry exam, making it necessary to evaluate risk factors other than bone density. In this context, the FRAX (Fracture Risk Assessment Tool) tool brings together other risk factors for fracture prediction independent of BMD, such as the presence of previous fragility fracture, hip fragility fracture in the parents, current smoking, use of glucocorticoids, rheumatoid arthritis, secondary osteoporosis, and use of three or more units of alcoholic beverage per day1-4. Interestingly, FRAX is an algorithm that analyzes all clinical risk factors together and finally calculates the absolute risk of fracture in 10 years. Patients diagnosed with osteoporosis or those at high risk of fracture by FRAX deserve drug treatment targeting bone mass gain and fracture prevention. Among the drug strategies are anti-resorptive drugs (bisphosphonates and denosumab) and anabolic agents (teriparatide and romosozumab), which must be associated with other measures, such as physical activity, calcium intake, preferably in the diet, and supplementation of vitamin D2. The prevalence of osteoporosis increases with age, with a consequent increase in the number of fractures, either due to worsening of the bone structure, with thinning of the cortical bone, reduction of the trabeculae, and alteration of the bone microarchitecture, or due to the increased risk of falls, reduced lean mass, impairment of proprioception, and decreased visual acuity, among other factors. Osteoporotic fractures are those due to fragility, that is, low impact. Fragility fractures may be asymptomatic, mostly when occurred in the vertebral bodies with wedging, leading to height loss and dorsal hyperkyphosis5. Annually, almost 9 million fractures occur worldwide due to osteoporosis, which corresponds to an osteoporosis-related fracture every 3 s, and of these fractures, 1.6 million are hip fractures. The world estimate is that there are about 500 million people with osteoporosis, predominantly women, with an estimated fracture resulting from osteoporosis occurring in one in three women over 50 years and one in five men in the same age group5. BMD is directly related to fracture risk. The loss of 10% of BMD in the spine is associated with twice the risk of fracture, and the same loss of BMD in the hip leads to an increase in the risk of fracture by two and a half times. A previous fracture increases the risk of a new fracture by 86%, mainly in the subsequent 2 years. Despite the financial cost, morbidity, and mortality associated with osteoporosis, evidence shows that up to 80% of women with fragility fractures are not diagnosed or treated for osteoporosis5.
期刊介绍:
A Revista da Associação Médica Brasileira (RAMB), editada pela Associação Médica Brasileira, desde 1954, tem por objetivo publicar artigos que contribuam para o conhecimento médico.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
