Prem N Patel, Ahmed M Alkaliby, Mitul C Mehta, Angeline L Wang
{"title":"CMV retinitis in patients on mycophenolate immunosuppression: a report of two cases.","authors":"Prem N Patel, Ahmed M Alkaliby, Mitul C Mehta, Angeline L Wang","doi":"10.1186/s13223-023-00817-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The rate of cytomegalovirus (CMV) retinitis is increasing, likely secondary to aggressive immunosuppressive regimens for a variety of diseases. Transplant and rheumatological literature show growing evidence suggesting a unique relationship between CMV infection and mycophenolate in particular. This study reports two cases of CMV retinitis infection in patients on mycophenolate immunosuppression.</p><p><strong>Case presentation: </strong>Case A was a 39-year-old African American woman with systemic lupus erythematosus (SLE) with stage IV lupus nephritis who presented for bilateral retinal detachments with areas of moth-eaten and thin retina concerning for prior viral retinitis. Case B was a 53-year-old man who presented with floaters in the right eye status-post heart transplant since 2008 on immunosuppressive therapy. Fundoscopic examination of the right eye showed frosted branch angiitis with intraretinal hemorrhage and inner retinal thickening and disorganization, consistent with CMV retinitis infection. Both patients were on mycophenolate immunosuppression with the recommendation to reduce or discontinue mycophenolate.</p><p><strong>Conclusion: </strong>Patients on mycophenolate immunosuppression may be more vulnerable to cytomegalovirus infection, including CMV retinitis. Ophthalmologists should be aware of this increased risk and consider reducing or discontinuing mycophenolate to promote viral clearance in these susceptible patients, in conjunction with the patient's transplant or rheumatology teams.</p>","PeriodicalId":7702,"journal":{"name":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","volume":"19 1","pages":"72"},"PeriodicalIF":0.0000,"publicationDate":"2023-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10440026/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13223-023-00817-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The rate of cytomegalovirus (CMV) retinitis is increasing, likely secondary to aggressive immunosuppressive regimens for a variety of diseases. Transplant and rheumatological literature show growing evidence suggesting a unique relationship between CMV infection and mycophenolate in particular. This study reports two cases of CMV retinitis infection in patients on mycophenolate immunosuppression.
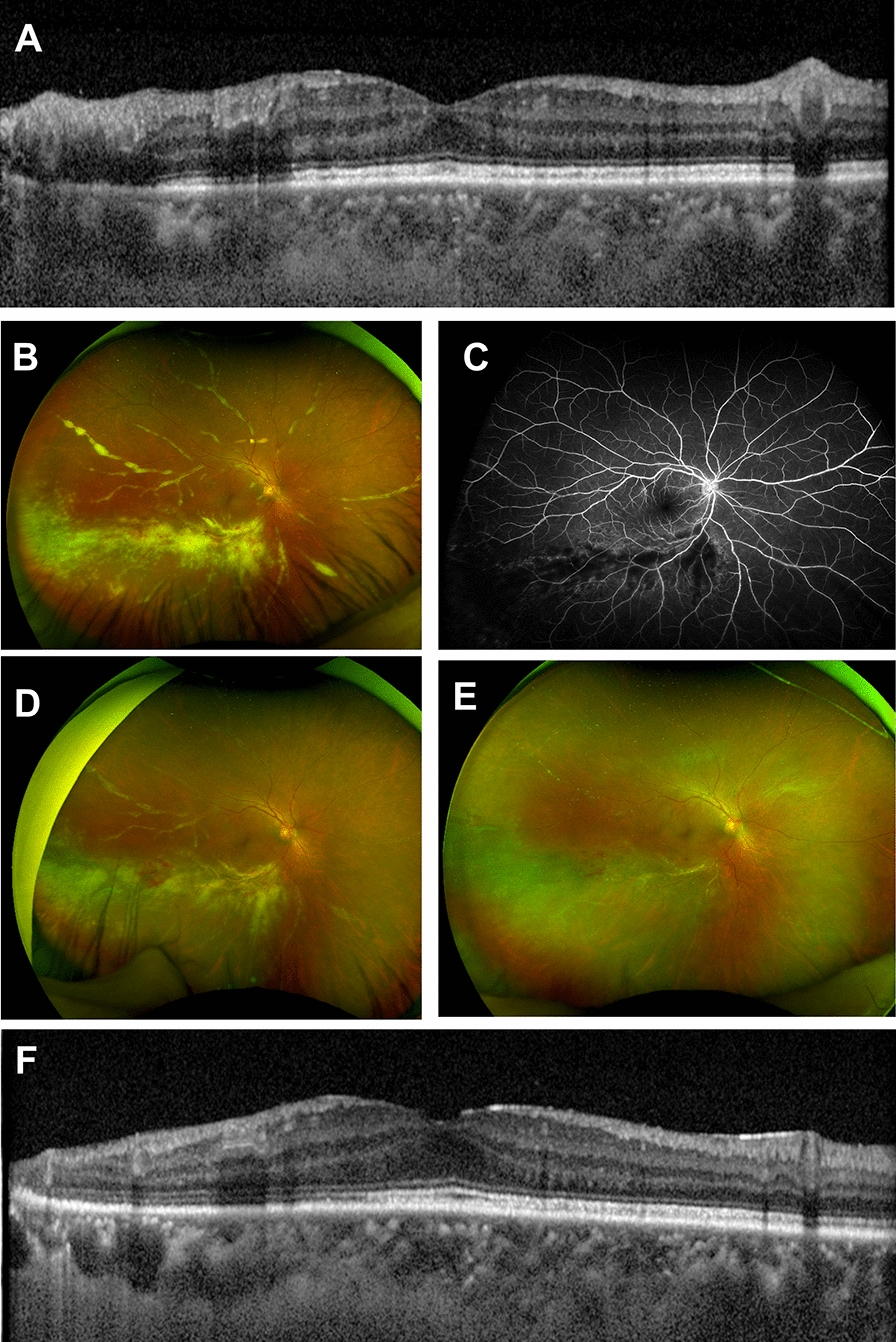
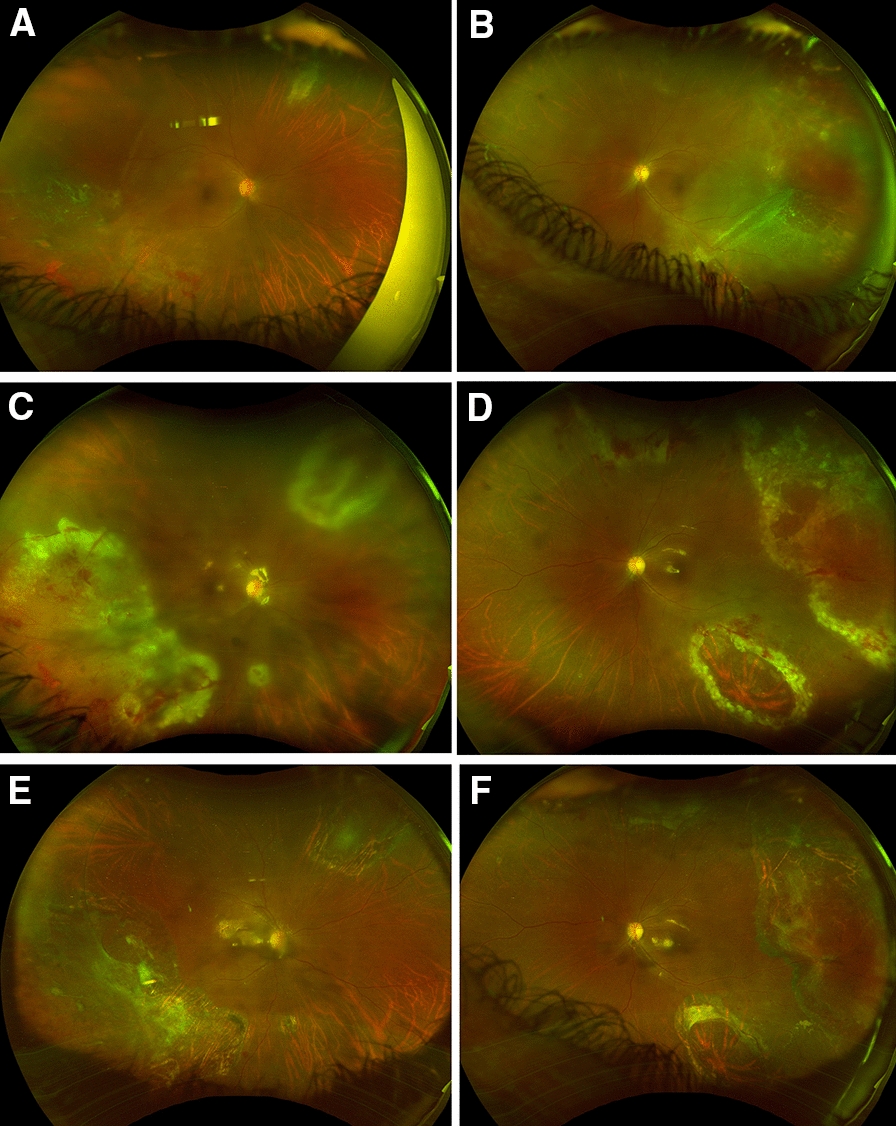
Case presentation: Case A was a 39-year-old African American woman with systemic lupus erythematosus (SLE) with stage IV lupus nephritis who presented for bilateral retinal detachments with areas of moth-eaten and thin retina concerning for prior viral retinitis. Case B was a 53-year-old man who presented with floaters in the right eye status-post heart transplant since 2008 on immunosuppressive therapy. Fundoscopic examination of the right eye showed frosted branch angiitis with intraretinal hemorrhage and inner retinal thickening and disorganization, consistent with CMV retinitis infection. Both patients were on mycophenolate immunosuppression with the recommendation to reduce or discontinue mycophenolate.
Conclusion: Patients on mycophenolate immunosuppression may be more vulnerable to cytomegalovirus infection, including CMV retinitis. Ophthalmologists should be aware of this increased risk and consider reducing or discontinuing mycophenolate to promote viral clearance in these susceptible patients, in conjunction with the patient's transplant or rheumatology teams.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
