Ja Min Byun, Sung-Soo Park, Sung-Soo Yoon, Ari Ahn, Myungshin Kim, Jung Yeon Lee, Young-Woo Jeon, Seung-Hwan Shin, Seung-Ah Yahng, Youngil Koh, Chang-Ki Min
{"title":"Advantage of achieving deep response following frontline daratumumab-VTd compared to VRd in transplant-eligible multiple myeloma: multicenter study.","authors":"Ja Min Byun, Sung-Soo Park, Sung-Soo Yoon, Ari Ahn, Myungshin Kim, Jung Yeon Lee, Young-Woo Jeon, Seung-Hwan Shin, Seung-Ah Yahng, Youngil Koh, Chang-Ki Min","doi":"10.5045/br.2023.2023005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The goal of induction therapy for multiple myeloma (MM) is to achieve adequate disease control. Current guidelines favor triplet (bortezomib-lenalidomide-dexamethasone; VRd) or quadruplet regimens (daratumumab, bortezomib-thalidomide-dexamethasone; D-VTd). In the absence of a direct comparison between two treatment regimens, we conducted this study to compare the outcomes and safety of VRd and D-VTd.</p><p><strong>Methods: </strong>Newly diagnosed MM patients aged >18 years who underwent induction therapy followed by autologous stem cell transplantation (ASCT) between November 2020 and December 2021 were identified. Finally, patients with VRd (N=37) and those with D-VTd (N=43) were enrolled.</p><p><strong>Results: </strong>After induction, 10.8% of the VRd group showed stringent complete remission (sCR), 21.6% showed complete response (CR), 35.1% showed very good partial response (VGPR), and 32.4% showed partial response (PR). Of the D-VTd group, 9.3% showed sCR, 34.9% CR, 48.8% VGPR, and 4.2% PR (VGPR or better: 67.6% in VRd vs. 93% in D-VTd, P=0.004). After ASCT, 68.6% of the VRd group showed CR or sCR, while 90.5% of the D-VTd group showed CR or sCR (P=0.016). VRd was associated with an increased incidence of skin rash (P=0.044). Other than rashes, there were no significant differences in terms of adverse events between the two groups.</p><p><strong>Conclusion: </strong>Our study supports the use of a front-line quadruplet induction regimen containing a CD38 monoclonal antibody for transplant-eligible patients with newly diagnosed MM.</p>","PeriodicalId":46224,"journal":{"name":"Blood Research","volume":"58 2","pages":"83-90"},"PeriodicalIF":2.8000,"publicationDate":"2023-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/ef/br-58-2-83.PMC10310489.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Blood Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5045/br.2023.2023005","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The goal of induction therapy for multiple myeloma (MM) is to achieve adequate disease control. Current guidelines favor triplet (bortezomib-lenalidomide-dexamethasone; VRd) or quadruplet regimens (daratumumab, bortezomib-thalidomide-dexamethasone; D-VTd). In the absence of a direct comparison between two treatment regimens, we conducted this study to compare the outcomes and safety of VRd and D-VTd.
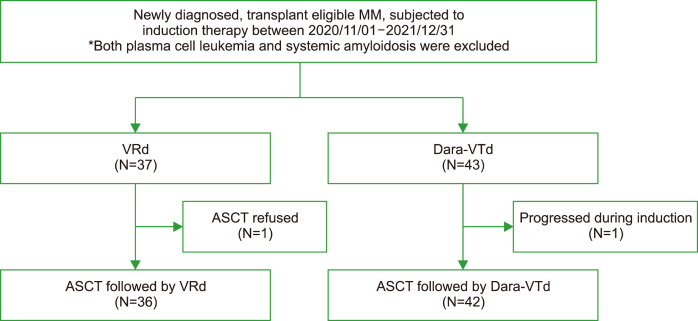
Methods: Newly diagnosed MM patients aged >18 years who underwent induction therapy followed by autologous stem cell transplantation (ASCT) between November 2020 and December 2021 were identified. Finally, patients with VRd (N=37) and those with D-VTd (N=43) were enrolled.
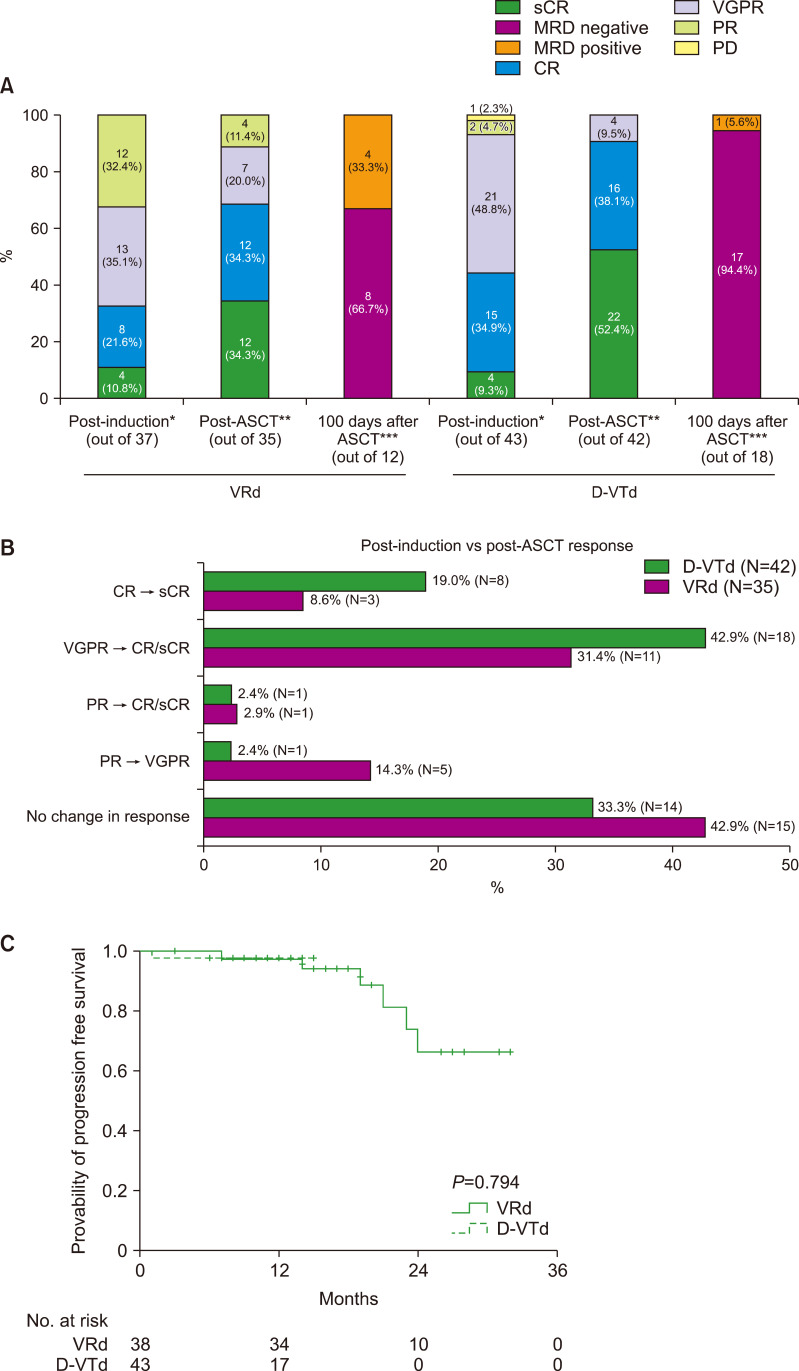
Results: After induction, 10.8% of the VRd group showed stringent complete remission (sCR), 21.6% showed complete response (CR), 35.1% showed very good partial response (VGPR), and 32.4% showed partial response (PR). Of the D-VTd group, 9.3% showed sCR, 34.9% CR, 48.8% VGPR, and 4.2% PR (VGPR or better: 67.6% in VRd vs. 93% in D-VTd, P=0.004). After ASCT, 68.6% of the VRd group showed CR or sCR, while 90.5% of the D-VTd group showed CR or sCR (P=0.016). VRd was associated with an increased incidence of skin rash (P=0.044). Other than rashes, there were no significant differences in terms of adverse events between the two groups.
Conclusion: Our study supports the use of a front-line quadruplet induction regimen containing a CD38 monoclonal antibody for transplant-eligible patients with newly diagnosed MM.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
