{"title":"Separation Surgery and Adjuvant Carbon Ion Radiotherapy for a Recurrent Solitary Fibrous Tumor/Hemangiopericytoma: A Case Report.","authors":"Yusuke Tomomatsu, Eiji Takasawa, Shintaro Shiba, Masahiko Okamoto, Hayato Ikota, Kazuhiro Inomata, Akira Honda, Sho Ishiwata, Tokue Mieda, Yoichi Iizuka, Tatsuya Ohno, Hirotaka Chikuda","doi":"10.22603/ssrr.2022-0177","DOIUrl":null,"url":null,"abstract":"The treatment of solitary fibrous tumor/hemangiopericytoma (SFT/HPC) remains challenging because gross total resection is difficult for vertebral lesions located near the spinal cord. Adjuvant chemotherapy and radiotherapy can be considered for cases of recurrence or malignant change. We herein report our experience of performing separation surgery and adjuvant carbon ion radiotherapy (CIRT) for a rare case of recurrent spinal SFT/HPC. Ten years ago, a 74-year-old woman visited a public hospital with a 2-month history of chest pain, muscle weakness, and hypesthesia in her lower extremities. Magnetic resonance imaging (MRI) revealed an extradural, extramedullary dumbbell-shaped tumor at the T4-T5 level (Fig. 1-A). She underwent subtotal tumor resection combined with T2-T7 fusion. Pathological examination of the resected specimen revealed SFT/HPC grade 3. Seven years after the initial surgery, she was referred to our university hospital because of unsteady gait due to progressive thoracic myelopathy. Imaging studies showed local recurrence of the tumor. We performed partial resection of the tumor surrounding the dural sac because total resection was considered to have a high risk of spinal cord injury. Postoperatively, she was able to walk without support. Two years after her second operation, she gradually became bedridden due to progressive gait disturbance with dysesthesia below the T5 level. MRI showed spinal cord compression due to the regrowth of the recurrent tumor with vertebral invasion (Fig. 1-B). We planned separation surgery and adjuvant CIRT. Following additional laminectomy, the tumor was observed as a nodular, tan to reddish-brown mass, which surrounded the dura mater. An ultrasonic scalpel was used to remove the tumor adjacent to the dural sac. Gelfoam of 1-cm thickness wrapped with Goa-Tex membrane (Fig. 2-A) was placed between the ventral dura mater and the residual tumor as a spacer (Fig. 2-B). We then applied 5.5-mm Ti-alloy rods medially to allow for the optimal trajectory of irradiation (Fig. 2-C). After separation surgery, adjuvant CIRT was performed once a day, 4 days per week, in a total of 16 fractions over 4 weeks with the respiratory-gated plan (Fig. 3-B) for a total dose of 64.0 Gy. Two years after separation surgery and adjuvant CIRT, the tumor size had decreased, and local control was maintained (Fig. 3-C, 3-D). The patient was able to walk with a cane without CIRT-related adverse events. Histopathological examination revealed spindle cells proliferating with staghorn-like shaped vessels (Fig. 4-A, 4-B). According to immunohistochemistry, the intervening blood vessels expressed biomarkers CD34, and tumor cells were positive for the nuclear marker STAT6, indicating SFT (Fig. 4-C, 4-D). The final diagnosis was SFT/HPC grade 3. The local control rates of SFT/HPC treated with gross total and subtotal resection are reported to be 84% and 30%, respectively, with a time to recurrence of approximately 5 years. Although CIRT is a potential additional treatment option for recurrent SFT/HPC, there is only one report of CIRT combined with separation surgery. In our case, the","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 4","pages":"402-405"},"PeriodicalIF":1.2000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cb/00/2432-261X-7-0402.PMC10447192.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0177","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
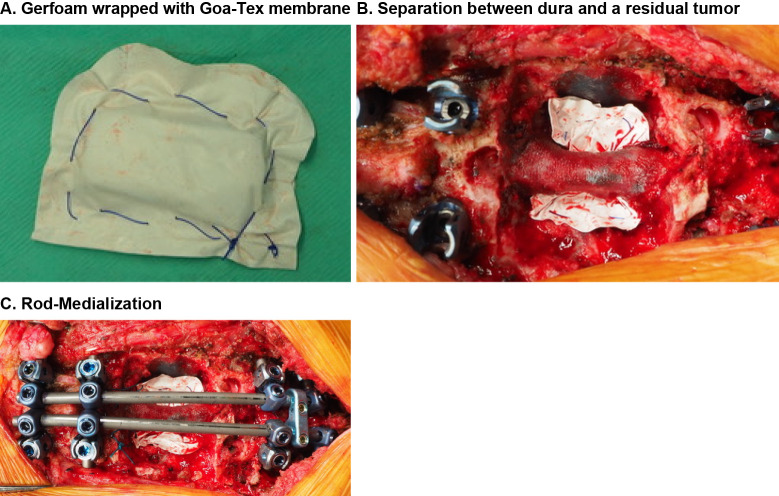
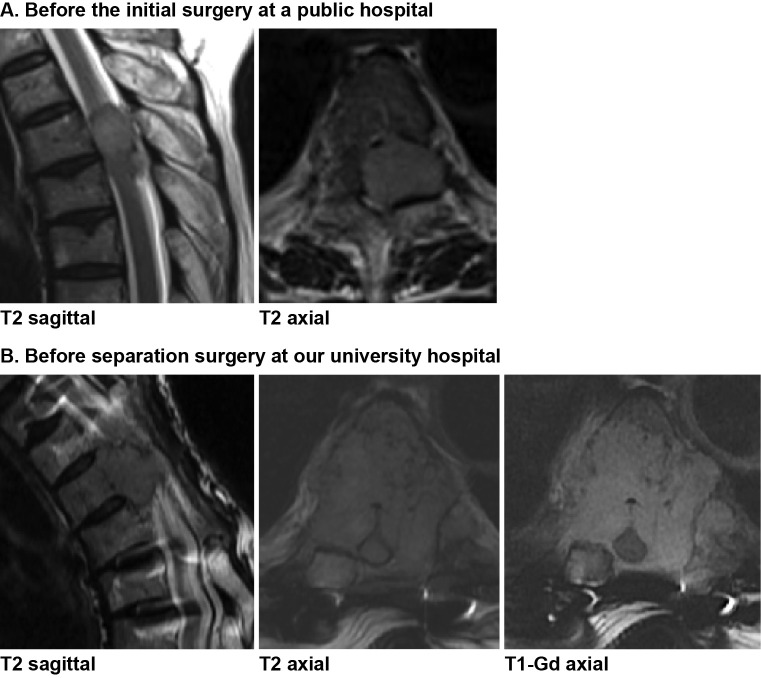
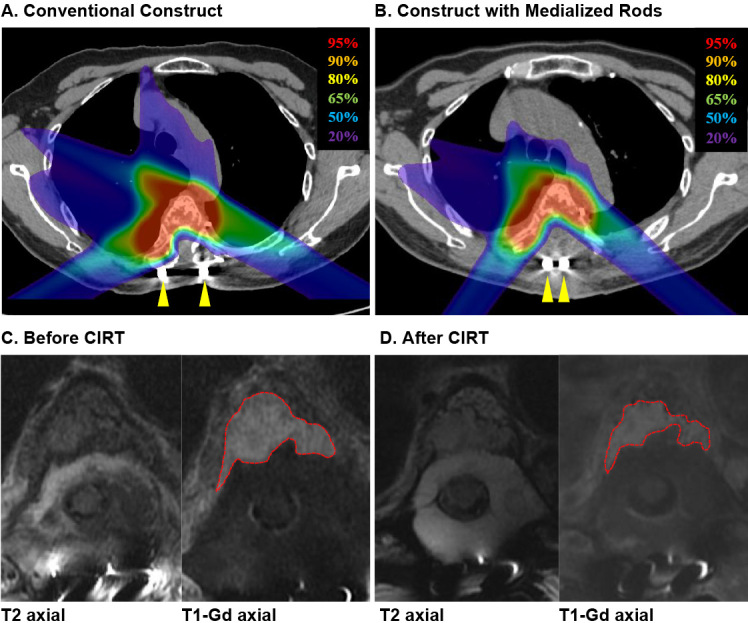
The treatment of solitary fibrous tumor/hemangiopericytoma (SFT/HPC) remains challenging because gross total resection is difficult for vertebral lesions located near the spinal cord. Adjuvant chemotherapy and radiotherapy can be considered for cases of recurrence or malignant change. We herein report our experience of performing separation surgery and adjuvant carbon ion radiotherapy (CIRT) for a rare case of recurrent spinal SFT/HPC. Ten years ago, a 74-year-old woman visited a public hospital with a 2-month history of chest pain, muscle weakness, and hypesthesia in her lower extremities. Magnetic resonance imaging (MRI) revealed an extradural, extramedullary dumbbell-shaped tumor at the T4-T5 level (Fig. 1-A). She underwent subtotal tumor resection combined with T2-T7 fusion. Pathological examination of the resected specimen revealed SFT/HPC grade 3. Seven years after the initial surgery, she was referred to our university hospital because of unsteady gait due to progressive thoracic myelopathy. Imaging studies showed local recurrence of the tumor. We performed partial resection of the tumor surrounding the dural sac because total resection was considered to have a high risk of spinal cord injury. Postoperatively, she was able to walk without support. Two years after her second operation, she gradually became bedridden due to progressive gait disturbance with dysesthesia below the T5 level. MRI showed spinal cord compression due to the regrowth of the recurrent tumor with vertebral invasion (Fig. 1-B). We planned separation surgery and adjuvant CIRT. Following additional laminectomy, the tumor was observed as a nodular, tan to reddish-brown mass, which surrounded the dura mater. An ultrasonic scalpel was used to remove the tumor adjacent to the dural sac. Gelfoam of 1-cm thickness wrapped with Goa-Tex membrane (Fig. 2-A) was placed between the ventral dura mater and the residual tumor as a spacer (Fig. 2-B). We then applied 5.5-mm Ti-alloy rods medially to allow for the optimal trajectory of irradiation (Fig. 2-C). After separation surgery, adjuvant CIRT was performed once a day, 4 days per week, in a total of 16 fractions over 4 weeks with the respiratory-gated plan (Fig. 3-B) for a total dose of 64.0 Gy. Two years after separation surgery and adjuvant CIRT, the tumor size had decreased, and local control was maintained (Fig. 3-C, 3-D). The patient was able to walk with a cane without CIRT-related adverse events. Histopathological examination revealed spindle cells proliferating with staghorn-like shaped vessels (Fig. 4-A, 4-B). According to immunohistochemistry, the intervening blood vessels expressed biomarkers CD34, and tumor cells were positive for the nuclear marker STAT6, indicating SFT (Fig. 4-C, 4-D). The final diagnosis was SFT/HPC grade 3. The local control rates of SFT/HPC treated with gross total and subtotal resection are reported to be 84% and 30%, respectively, with a time to recurrence of approximately 5 years. Although CIRT is a potential additional treatment option for recurrent SFT/HPC, there is only one report of CIRT combined with separation surgery. In our case, the



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
