{"title":"Ureter Injury in Total Laparoscopic Hysterectomy.","authors":"Hiroharu Kobayashi, Aimi Oda, Yoshihiko Matsuzaki, Yuki Kondo, Yuri Hamada, Masaru Nagashima, Misa Kobayashi, Yoshihiro Takaki, Hiroshi Adachi","doi":"10.1155/2023/5071080","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To identify surgical manipulations that caused ureter injury during total laparoscopic hysterectomy (TLH) and evaluate the surgical manipulations to identify ways to prevent such injury. <i>Patients and Methods</i>. This single-center, cross-sectional study included 1135 cases of TLH performed for benign diseases from January 2009 to December 2021. Seven cases (0.6%) that needed ureteral stent placement intra- or postoperatively for ureter injury were included. We identified the surgical manipulations that caused ureter injury from surgical videos.</p><p><strong>Results: </strong>Two cases had adhesions around the bladder pillar, and the ureter sustained a thermal injury during the cardinal ligament transection. One case had severe endometriosis, and the ureter was bluntly damaged when the adhesion was released. In one case, the ureter was thermally damaged during bipolar hemostasis for uterine artery bleeding. In two cases, the obliterated umbilical artery was mistaken for the ureter, and the real ureter was injured. In one case, ureteral peristalsis was inhibited by a pelvic abscess caused by postoperative infection.</p><p><strong>Conclusion: </strong>To prevent ureter injury during TLH, the ureter should be isolated in case of severe adhesion. Moreover, the following could be considered: (1) expand Okabayashi's pararectal space lateral to the uterosacral ligament, (2) perform dissection sharply using a monopolar or scissors forceps when releasing adhesion, (3) clarify the anatomy around the ureter for cases needing hemostasis, (4) repeatedly confirm the ureter with its peristalsis even after its isolation, (5) for severe adhesion cases, reduce infection risk by drain placement and administering antibiotics, and (6) use a delineator cup.</p>","PeriodicalId":9610,"journal":{"name":"Case Reports in Obstetrics and Gynecology","volume":"2023 ","pages":"5071080"},"PeriodicalIF":0.8000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10457165/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Obstetrics and Gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2023/5071080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To identify surgical manipulations that caused ureter injury during total laparoscopic hysterectomy (TLH) and evaluate the surgical manipulations to identify ways to prevent such injury. Patients and Methods. This single-center, cross-sectional study included 1135 cases of TLH performed for benign diseases from January 2009 to December 2021. Seven cases (0.6%) that needed ureteral stent placement intra- or postoperatively for ureter injury were included. We identified the surgical manipulations that caused ureter injury from surgical videos.
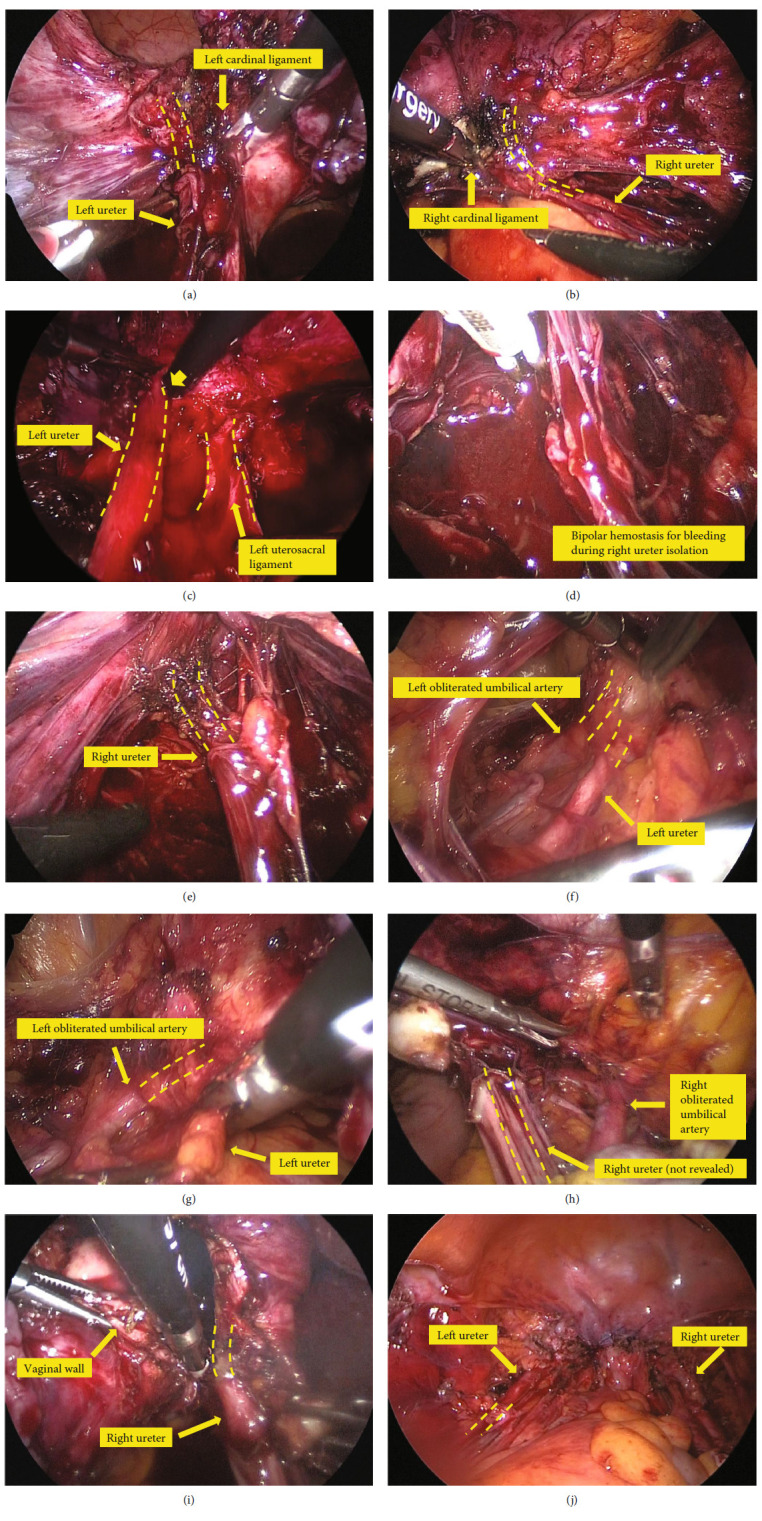
Results: Two cases had adhesions around the bladder pillar, and the ureter sustained a thermal injury during the cardinal ligament transection. One case had severe endometriosis, and the ureter was bluntly damaged when the adhesion was released. In one case, the ureter was thermally damaged during bipolar hemostasis for uterine artery bleeding. In two cases, the obliterated umbilical artery was mistaken for the ureter, and the real ureter was injured. In one case, ureteral peristalsis was inhibited by a pelvic abscess caused by postoperative infection.
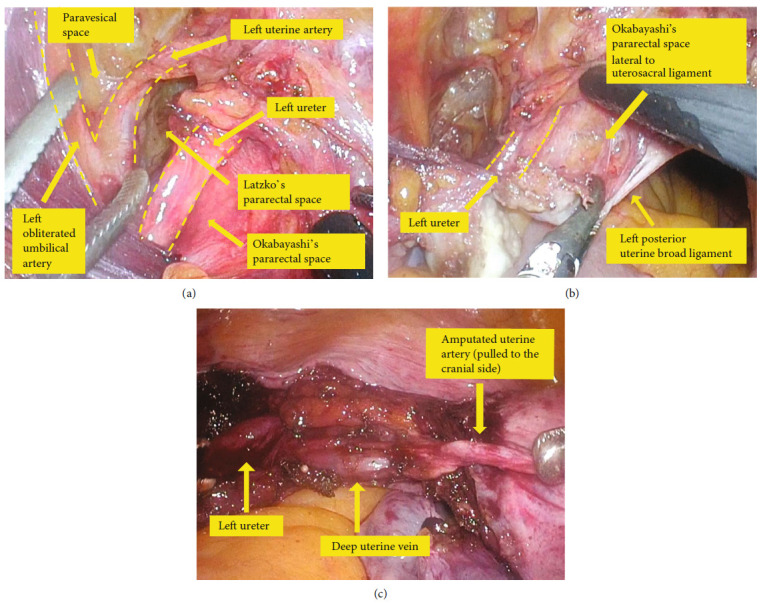
Conclusion: To prevent ureter injury during TLH, the ureter should be isolated in case of severe adhesion. Moreover, the following could be considered: (1) expand Okabayashi's pararectal space lateral to the uterosacral ligament, (2) perform dissection sharply using a monopolar or scissors forceps when releasing adhesion, (3) clarify the anatomy around the ureter for cases needing hemostasis, (4) repeatedly confirm the ureter with its peristalsis even after its isolation, (5) for severe adhesion cases, reduce infection risk by drain placement and administering antibiotics, and (6) use a delineator cup.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
