{"title":"Risk Factors for Cage Subsidence in Minimally Invasive Lateral Corpectomy for Osteoporotic Vertebral Fractures.","authors":"Shuhei Iwata, Toshiaki Kotani, Tsuyoshi Sakuma, Yasushi Iijima, Shun Okuwaki, Shuhei Ohyama, Satoshi Maki, Yawara Eguchi, Sumihisa Orita, Kazuhide Inage, Yasuhiro Shiga, Masahiro Inoue, Tsutomu Akazawa, Shohei Minami, Seiji Ohtori","doi":"10.22603/ssrr.2022-0215","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>This study aims to investigate risk factors for cage subsidence following minimally invasive lateral corpectomy for osteoporotic vertebral fractures.</p><p><strong>Methods: </strong>Eight males and 13 females (77.2±6.0 years old) with osteoporotic vertebral fractures who underwent single corpectomy using a wide-footprint expandable cage with at least a 1-year follow-up were retrospectively included. The endplate cage (EC) angle was defined as the angle between the vertebral body's endplate and the cage's base on the cranial and caudal sides. A sagittal computed tomography scan was performed immediately after surgery and at the final follow-up, with cage subsidence defined as subsidence of ≥2 mm on the cranial or caudal side. Risk factors were analyzed by dividing cases into groups with (<i>n</i>=6) and without (<i>n</i>=15) cage subsidence.</p><p><strong>Results: </strong>No significant differences were noted in age, bone mineral density, number of fixed vertebrae, sagittal parameters, preoperative and final kyphosis angle, amount of kyphosis angle correction, bone union, screw loosening, and number of other vertebral fractures preoperatively and 1-year postoperatively between the two groups. No difference was noted in cranial EC angle, but a significant difference was noted in caudal EC angle in the group with (10.7±4.1°) and without (4.7±4.2°) subsidence (<i>P</i>=0.008). Logistic regression analysis with the dependent variable as presence or absence of subsidence showed that caudal EC angle (>7.5°) was a significant factor (odds ratio: 20, 95% confidence interval: 1.655-241.7, <i>P</i>=0.018).</p><p><strong>Conclusions: </strong>In minimally invasive lateral corpectomy for osteoporotic vertebral fractures, a cage tilted more than 7.5° to the caudal vertebral endplate is a risk factor for cage subsidence. The cage should be placed as perpendicular to the endplate as possible, especially to the caudal vertebral body, to avoid cage subsidence.</p>","PeriodicalId":22253,"journal":{"name":"Spine Surgery and Related Research","volume":"7 4","pages":"356-362"},"PeriodicalIF":1.2000,"publicationDate":"2023-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/ac/10/2432-261X-7-0356.PMC10447195.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Spine Surgery and Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22603/ssrr.2022-0215","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: This study aims to investigate risk factors for cage subsidence following minimally invasive lateral corpectomy for osteoporotic vertebral fractures.
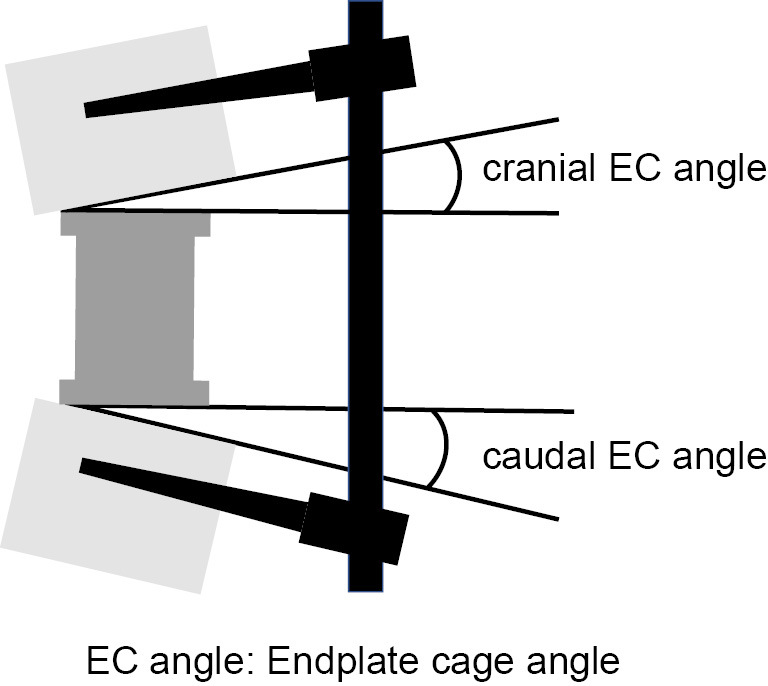
Methods: Eight males and 13 females (77.2±6.0 years old) with osteoporotic vertebral fractures who underwent single corpectomy using a wide-footprint expandable cage with at least a 1-year follow-up were retrospectively included. The endplate cage (EC) angle was defined as the angle between the vertebral body's endplate and the cage's base on the cranial and caudal sides. A sagittal computed tomography scan was performed immediately after surgery and at the final follow-up, with cage subsidence defined as subsidence of ≥2 mm on the cranial or caudal side. Risk factors were analyzed by dividing cases into groups with (n=6) and without (n=15) cage subsidence.
Results: No significant differences were noted in age, bone mineral density, number of fixed vertebrae, sagittal parameters, preoperative and final kyphosis angle, amount of kyphosis angle correction, bone union, screw loosening, and number of other vertebral fractures preoperatively and 1-year postoperatively between the two groups. No difference was noted in cranial EC angle, but a significant difference was noted in caudal EC angle in the group with (10.7±4.1°) and without (4.7±4.2°) subsidence (P=0.008). Logistic regression analysis with the dependent variable as presence or absence of subsidence showed that caudal EC angle (>7.5°) was a significant factor (odds ratio: 20, 95% confidence interval: 1.655-241.7, P=0.018).
Conclusions: In minimally invasive lateral corpectomy for osteoporotic vertebral fractures, a cage tilted more than 7.5° to the caudal vertebral endplate is a risk factor for cage subsidence. The cage should be placed as perpendicular to the endplate as possible, especially to the caudal vertebral body, to avoid cage subsidence.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
