{"title":"Management of the left subclavian artery during aortic arch replacement using a frozen elephant trunk approach: a review.","authors":"Vicente Orozco-Sevilla, Joseph S Coselli","doi":"10.21037/cdt-22-248","DOIUrl":null,"url":null,"abstract":"<p><p>The frozen elephant trunk (FET) technique for total aortic arch replacement extends repair into the proximal portion of the descending thoracic aorta. Several techniques and modifications of total arch replacement have been described in the literature, and many of these iterations are related to facilitating the distal anastomosis while preserving flow to the left subclavian artery (LSCA), as well as maintaining posterior circulation of the brain via the vertebral artery, by reducing the circulatory arrest time during reconstruction. Because of the LSCA's posterior and deep anatomic location in the chest, particularly in obese patients, this revascularization is often challenging; additional concerns regarding LSCA revascularization include patients with large aortic arch aneurysms, those with dissected or calcified arteries, and reoperation. A careful plan for reconstruction is necessary. Whether revascularization is performed preoperative, intraoperative, or postoperatively, every effort should be made to include the left subclavian artery as part of the operational approach. Revascularization techniques include reimplantation as part of the island patch or direct anastomosis, stenting, bypass, transposition or a hybrid approach. The importance of maintaining circulation of the LSCA cannot be overstated. Preserving flow to the spinal cord via collaterals minimizes the risk of cord injury during FET procedure. In patients with a patent left internal mammary artery bypass, left arm arteriovenous fistula for hemodialysis, dominant circulation, or direct aortic origin of the left vertebral artery, revascularization is necessary as well. In the case of initial sacrifice, arm claudication or steal syndrome usually dictates delayed extra-anatomic revascularization in the postoperative period.</p>","PeriodicalId":9592,"journal":{"name":"Cardiovascular diagnosis and therapy","volume":"13 4","pages":"736-742"},"PeriodicalIF":2.1000,"publicationDate":"2023-08-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/62/cdt-13-04-736.PMC10478019.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiovascular diagnosis and therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/cdt-22-248","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
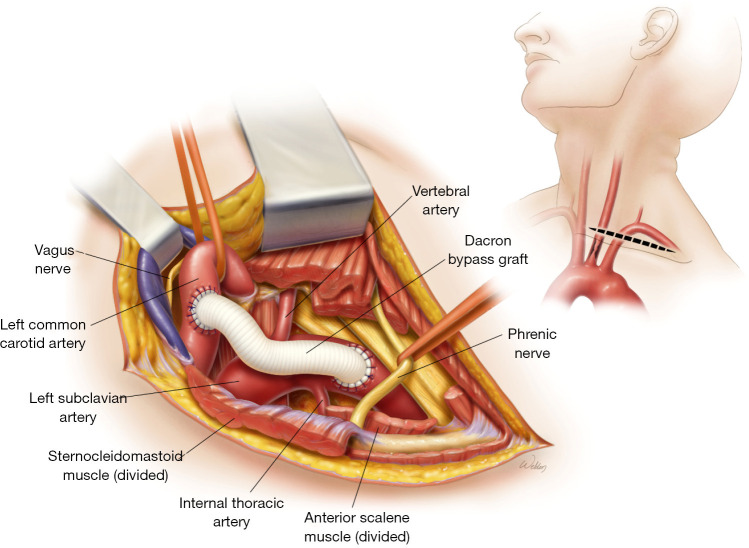
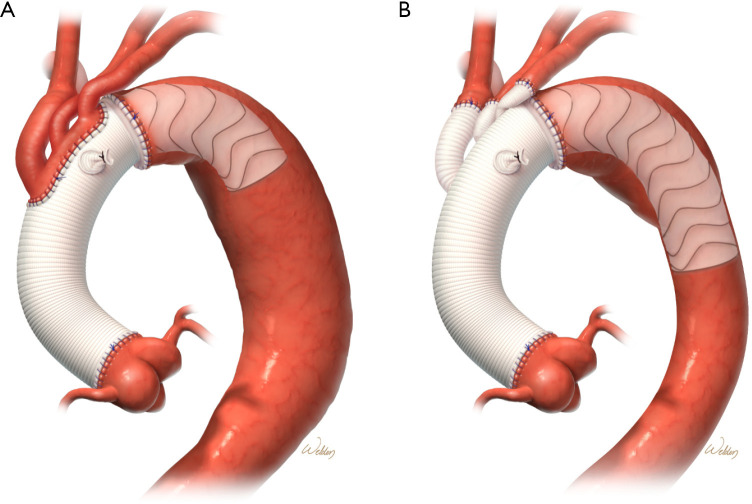
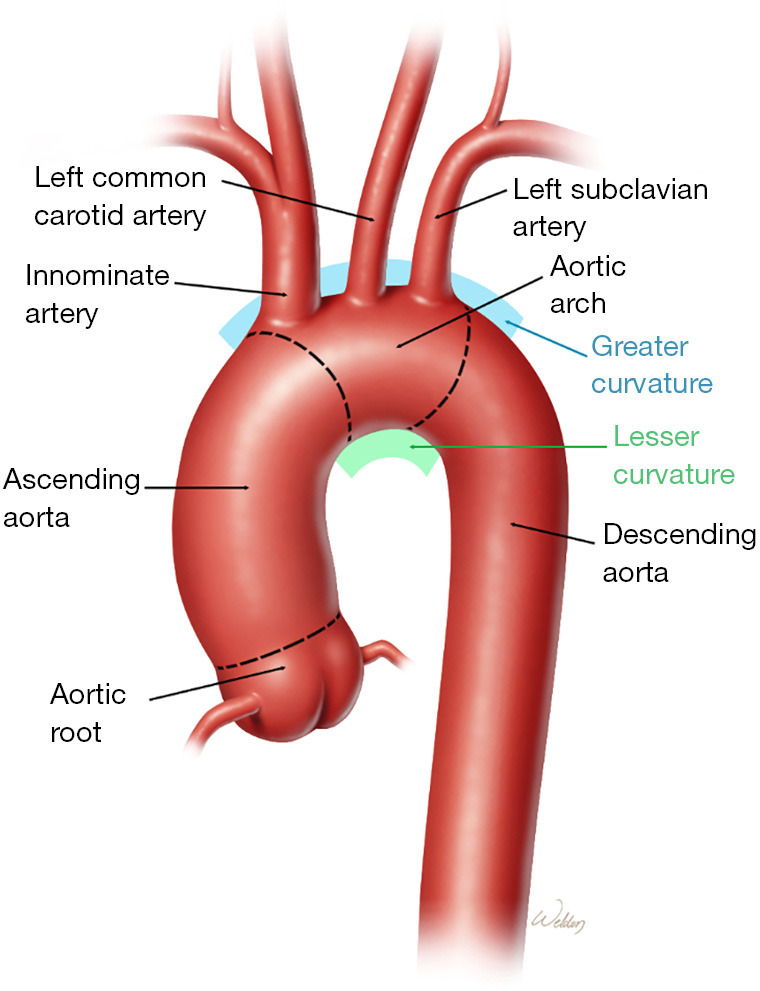
The frozen elephant trunk (FET) technique for total aortic arch replacement extends repair into the proximal portion of the descending thoracic aorta. Several techniques and modifications of total arch replacement have been described in the literature, and many of these iterations are related to facilitating the distal anastomosis while preserving flow to the left subclavian artery (LSCA), as well as maintaining posterior circulation of the brain via the vertebral artery, by reducing the circulatory arrest time during reconstruction. Because of the LSCA's posterior and deep anatomic location in the chest, particularly in obese patients, this revascularization is often challenging; additional concerns regarding LSCA revascularization include patients with large aortic arch aneurysms, those with dissected or calcified arteries, and reoperation. A careful plan for reconstruction is necessary. Whether revascularization is performed preoperative, intraoperative, or postoperatively, every effort should be made to include the left subclavian artery as part of the operational approach. Revascularization techniques include reimplantation as part of the island patch or direct anastomosis, stenting, bypass, transposition or a hybrid approach. The importance of maintaining circulation of the LSCA cannot be overstated. Preserving flow to the spinal cord via collaterals minimizes the risk of cord injury during FET procedure. In patients with a patent left internal mammary artery bypass, left arm arteriovenous fistula for hemodialysis, dominant circulation, or direct aortic origin of the left vertebral artery, revascularization is necessary as well. In the case of initial sacrifice, arm claudication or steal syndrome usually dictates delayed extra-anatomic revascularization in the postoperative period.
期刊介绍:
The journal ''Cardiovascular Diagnosis and Therapy'' (Print ISSN: 2223-3652; Online ISSN: 2223-3660) accepts basic and clinical science submissions related to Cardiovascular Medicine and Surgery. The mission of the journal is the rapid exchange of scientific information between clinicians and scientists worldwide. To reach this goal, the journal will focus on novel media, using a web-based, digital format in addition to traditional print-version. This includes on-line submission, review, publication, and distribution. The digital format will also allow submission of extensive supporting visual material, both images and video. The website www.thecdt.org will serve as the central hub and also allow posting of comments and on-line discussion. The web-site of the journal will be linked to a number of international web-sites (e.g. www.dxy.cn), which will significantly expand the distribution of its contents.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
