{"title":"Neonatal Intensive Care Unit to Home Discharge Communication: A Quality Improvement Project.","authors":"Priyam Pattnaik, Suhas Nafday, Robert Angert","doi":"10.1097/pq9.0000000000000669","DOIUrl":null,"url":null,"abstract":"<p><p>Neonatal intensive care unit (NICU) graduates require complex services after discharge. The NICU discharge process at Children's Hospital at Montefiore-Weiler, Bronx, NY (CHAM-Weiler) lacked a system for routine primary care provider (PCP) notification. Here, we describe a quality improvement project to improve communication with PCPs to ensure communication of critical information and plans.</p><p><strong>Methods: </strong>We assembled a multidisciplinary team and collected baseline data on discharge communication frequency and quality. We used quality improvement tools to implement a higher-quality system. The outcome measure was the successful delivery of a standardized notification and discharge summary to a PCP. We collected qualitative data through multidisciplinary meetings and direct feedback. The balancing measures comprised additional time spent during the discharge process and relaying erroneous information. We used a run chart to track progress and drive change.</p><p><strong>Results: </strong>Baseline data indicated that 67% of PCPs did not receive notifications before discharge, and when PCPs did receive notifications, the discharge plans were unclear. PCP feedback led to proactive electronic communication and a standardized notification. The key driver diagram allowed the team to design interventions that led to sustainable change. After multiple Plan-Do-Study-Act cycles, delivery of electronic PCP notifications occurred more than 90% of the time. Surveys of pediatricians who received notifications indicated that the notifications were highly valued and aided in the transition of care for these at-risk patients.</p><p><strong>Conclusion: </strong>A multidisciplinary team, including community pediatricians, was key to improving the rate of PCP notification of NICU discharge to more than 90% and transmitting higher-quality information.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"8 4","pages":"e669"},"PeriodicalIF":1.1000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10332829/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000669","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Neonatal intensive care unit (NICU) graduates require complex services after discharge. The NICU discharge process at Children's Hospital at Montefiore-Weiler, Bronx, NY (CHAM-Weiler) lacked a system for routine primary care provider (PCP) notification. Here, we describe a quality improvement project to improve communication with PCPs to ensure communication of critical information and plans.
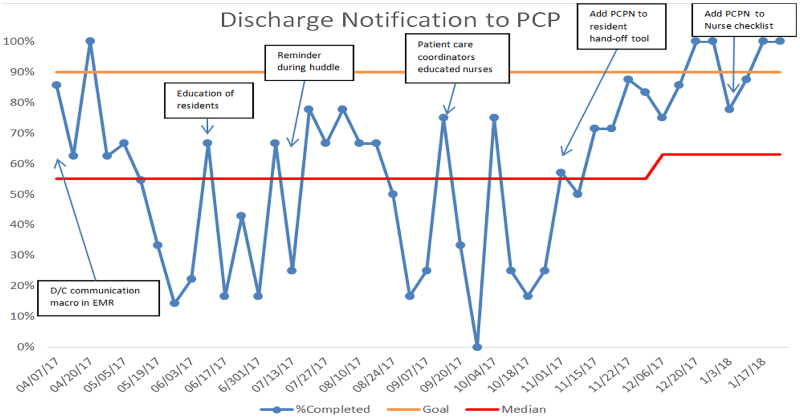
Methods: We assembled a multidisciplinary team and collected baseline data on discharge communication frequency and quality. We used quality improvement tools to implement a higher-quality system. The outcome measure was the successful delivery of a standardized notification and discharge summary to a PCP. We collected qualitative data through multidisciplinary meetings and direct feedback. The balancing measures comprised additional time spent during the discharge process and relaying erroneous information. We used a run chart to track progress and drive change.
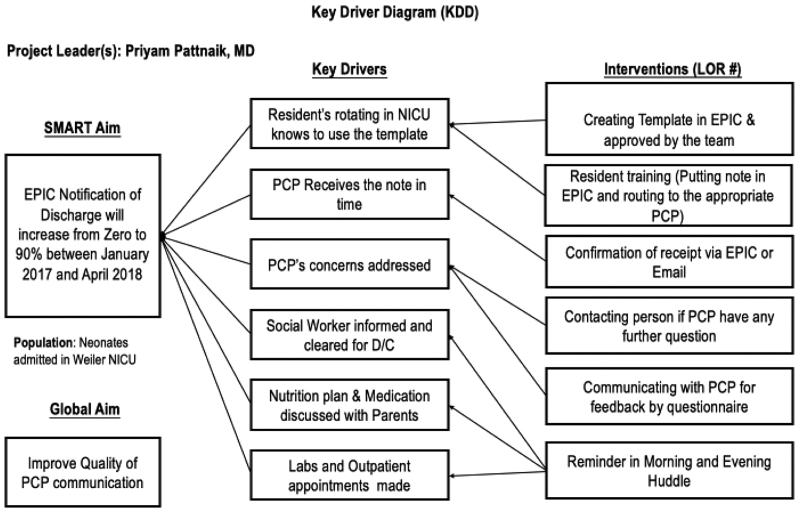
Results: Baseline data indicated that 67% of PCPs did not receive notifications before discharge, and when PCPs did receive notifications, the discharge plans were unclear. PCP feedback led to proactive electronic communication and a standardized notification. The key driver diagram allowed the team to design interventions that led to sustainable change. After multiple Plan-Do-Study-Act cycles, delivery of electronic PCP notifications occurred more than 90% of the time. Surveys of pediatricians who received notifications indicated that the notifications were highly valued and aided in the transition of care for these at-risk patients.
Conclusion: A multidisciplinary team, including community pediatricians, was key to improving the rate of PCP notification of NICU discharge to more than 90% and transmitting higher-quality information.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
