Bastian N Ruijter, Akin Inderson, Aad P van den Berg, Herold J Metselaar, Jeroen Dubbeld, Maarten E Tushuizen, Robert J Porte, Wojciech Polak, Danny van der Helm, Marjolein van Reeven, Mar Rodriguez-Girondo, Bart van Hoek
{"title":"Randomized Trial of Ciclosporin with 2-h Monitoring vs. Tacrolimus with Trough Monitoring in Liver Transplantation: DELTA Study.","authors":"Bastian N Ruijter, Akin Inderson, Aad P van den Berg, Herold J Metselaar, Jeroen Dubbeld, Maarten E Tushuizen, Robert J Porte, Wojciech Polak, Danny van der Helm, Marjolein van Reeven, Mar Rodriguez-Girondo, Bart van Hoek","doi":"10.14218/JCTH.2022.00348","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and aims: </strong>Previous trials comparing cyclosporine and tacrolimus after liver transplantation (LT) showed conflicting results. Most used trough monitoring for cyclosporine (C0), leading to less accurate dosing than with 2-h monitoring (C2). Only one larger trial compared C2 with tacrolimus based on trough level (T0) after LT, with similar treated biopsy-proven acute rejection (tBPAR) and graft loss, while a smaller trial had less tBPAR with C2 compared to T0. Therefore, it is still unclear which calcineurin inhibitor is preferred after LT. We aimed to demonstrate superior efficacy (tBPAR), tolerability, and safety of C2 or T0 after first LT.</p><p><strong>Methods: </strong>Patients after first LT were randomized to C2 or T0. tBPAR, patient- and graft survival, safety and tolerability were the main endpoints, with analysis by Fisher test, Kaplan-Meier survival analysis and log-rank test.</p><p><strong>Results: </strong>In intention-to-treat analysis 84 patients on C2 and 85 on T0 were included. Cumulative incidence of tBPAR C2 vs. T0 was 17.7% vs. 8.4% at 3 months (<i>p</i>=0.104), and 21.9% vs. 9.7% at 6 and 12 months (<i>p</i>=0.049). One-year cumulative mortality C2 vs. T0 was 15.5% vs. 5.9% (<i>p</i>=0.049) and graft loss 23.8% vs. 9.4% (<i>p</i>=0.015). Serum triglyceride and LDL-cholesterol was lower with T0 than with C2. Incidence of diarrhea in T0 vs, C2 was 64% vs. 31% (<i>p</i>≤0.001), with no other differences in safety and tolerability.</p><p><strong>Conclusions: </strong>In the first year after LT immunosuppression with T0 leads to less tBPAR and better patient-/re-transplant-free survival as compared to C2.</p>","PeriodicalId":15484,"journal":{"name":"Journal of Clinical and Translational Hepatology","volume":"11 4","pages":"839-849"},"PeriodicalIF":4.2000,"publicationDate":"2023-08-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/17/45/JCTH-11-839.PMC10318291.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical and Translational Hepatology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.14218/JCTH.2022.00348","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims: Previous trials comparing cyclosporine and tacrolimus after liver transplantation (LT) showed conflicting results. Most used trough monitoring for cyclosporine (C0), leading to less accurate dosing than with 2-h monitoring (C2). Only one larger trial compared C2 with tacrolimus based on trough level (T0) after LT, with similar treated biopsy-proven acute rejection (tBPAR) and graft loss, while a smaller trial had less tBPAR with C2 compared to T0. Therefore, it is still unclear which calcineurin inhibitor is preferred after LT. We aimed to demonstrate superior efficacy (tBPAR), tolerability, and safety of C2 or T0 after first LT.
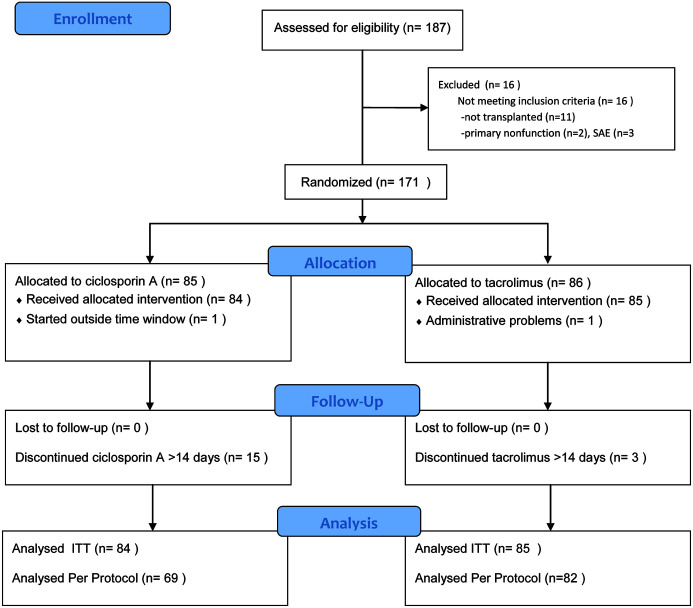
Methods: Patients after first LT were randomized to C2 or T0. tBPAR, patient- and graft survival, safety and tolerability were the main endpoints, with analysis by Fisher test, Kaplan-Meier survival analysis and log-rank test.
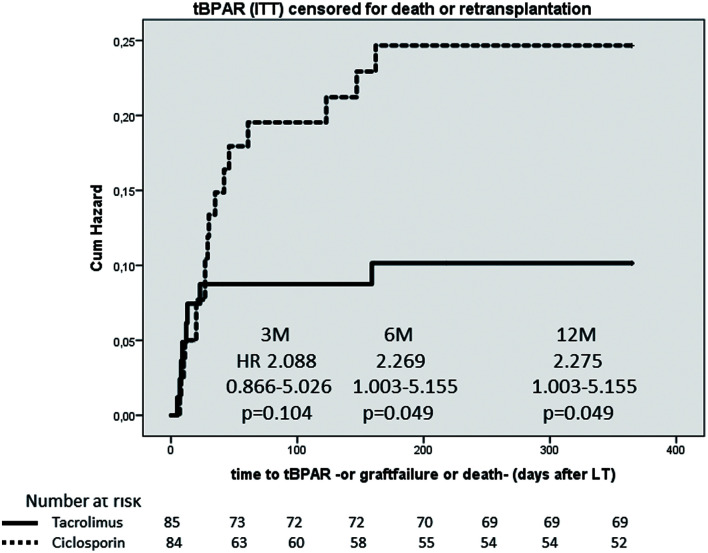
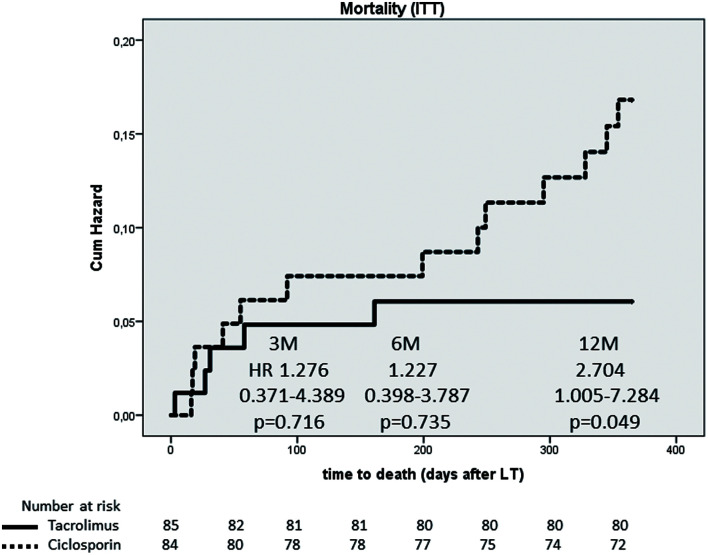
Results: In intention-to-treat analysis 84 patients on C2 and 85 on T0 were included. Cumulative incidence of tBPAR C2 vs. T0 was 17.7% vs. 8.4% at 3 months (p=0.104), and 21.9% vs. 9.7% at 6 and 12 months (p=0.049). One-year cumulative mortality C2 vs. T0 was 15.5% vs. 5.9% (p=0.049) and graft loss 23.8% vs. 9.4% (p=0.015). Serum triglyceride and LDL-cholesterol was lower with T0 than with C2. Incidence of diarrhea in T0 vs, C2 was 64% vs. 31% (p≤0.001), with no other differences in safety and tolerability.
Conclusions: In the first year after LT immunosuppression with T0 leads to less tBPAR and better patient-/re-transplant-free survival as compared to C2.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
