Hiroki Hori, Yusuke Yamada, Masayuki Nakano, Takahiro Ouchi, Masahito Takasaki, Ken Iijima, Takaomi Taira, Keiichi Abe, Hirokazu Iwamuro
{"title":"Improvement in Intraoperative Image Quality in Transcranial Magnetic Resonance-Guided Focused Ultrasound Surgery Using Transmitter Gain Adjustment.","authors":"Hiroki Hori, Yusuke Yamada, Masayuki Nakano, Takahiro Ouchi, Masahito Takasaki, Ken Iijima, Takaomi Taira, Keiichi Abe, Hirokazu Iwamuro","doi":"10.1159/000531009","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Transcranial magnetic resonance-guided focused ultrasound surgery (TcMRgFUS) has the advantage of allowing immediate evaluation of therapeutic effects after each sonication and intraoperative magnetic resonance imaging (MRI) to visualize the lesion. When the image shows that the lesion has missed the planned target and the therapeutic effects are insufficient, the target of the subsequent ablation can be finely adjusted based on the image. The precision of this adjustment is determined by the image quality. However, the current intraoperative image quality with a 3.0T MRI system is insufficient for precisely detecting the lesion. Thus, we developed and validated a method for improving intraoperative image quality.</p><p><strong>Methods: </strong>Because intraoperative image quality is affected by transmitter gain (TG), we acquired T2-weighted images (T2WIs) with two types of TG: the automatically adjusted TG (auto TG) and the manually adjusted TG (manual TG). To evaluate the character of images with 2 TGs, the actual flip angle (FA), the image uniformity, and the signal-to-noise ratio (SNR) were measured using a phantom. Then, to assess the quality of intraoperative images, T2WIs with both TGs were acquired during TcMRgFUS for 5 patients. The contrast-to-noise ratio (CNR) of the lesion was retrospectively estimated.</p><p><strong>Results: </strong>The images of the phantom with the auto TG showed substantial variations between the preset and actual FAs (p < 0.01), whereas on the images with the manual TG, there were no variations between the two FAs (p > 0.05). The total image uniformity was considerably lower with the manual TG than with the auto TG (p < 0.01), indicating that the image's signal values with the manual TG were more uniform. The manual TG produced significantly higher SNRs than the auto TG (p < 0.01). In the clinical study, the lesions were clearly detected in intraoperative images with the manual TG, but they were difficult to identify in images with the auto TG. The CNR of lesions in images with manual TG was considerably higher than in images with auto TG (p < 0.01).</p><p><strong>Conclusion: </strong>Regarding intraoperative T2WIs using a 3.0T MRI system during TcMRgFUS, the manual TG method improved image quality and delineated the ablative lesion more clearly than the current method with auto TG.</p>","PeriodicalId":22078,"journal":{"name":"Stereotactic and Functional Neurosurgery","volume":"101 4","pages":"223-231"},"PeriodicalIF":2.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10614472/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stereotactic and Functional Neurosurgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000531009","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/6/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"NEUROIMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Transcranial magnetic resonance-guided focused ultrasound surgery (TcMRgFUS) has the advantage of allowing immediate evaluation of therapeutic effects after each sonication and intraoperative magnetic resonance imaging (MRI) to visualize the lesion. When the image shows that the lesion has missed the planned target and the therapeutic effects are insufficient, the target of the subsequent ablation can be finely adjusted based on the image. The precision of this adjustment is determined by the image quality. However, the current intraoperative image quality with a 3.0T MRI system is insufficient for precisely detecting the lesion. Thus, we developed and validated a method for improving intraoperative image quality.
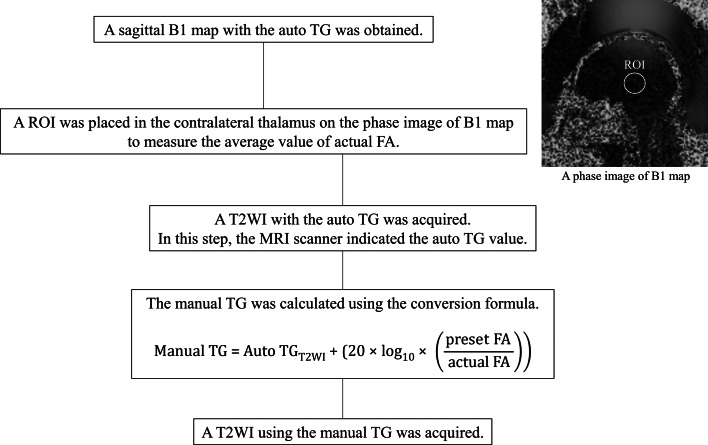
Methods: Because intraoperative image quality is affected by transmitter gain (TG), we acquired T2-weighted images (T2WIs) with two types of TG: the automatically adjusted TG (auto TG) and the manually adjusted TG (manual TG). To evaluate the character of images with 2 TGs, the actual flip angle (FA), the image uniformity, and the signal-to-noise ratio (SNR) were measured using a phantom. Then, to assess the quality of intraoperative images, T2WIs with both TGs were acquired during TcMRgFUS for 5 patients. The contrast-to-noise ratio (CNR) of the lesion was retrospectively estimated.
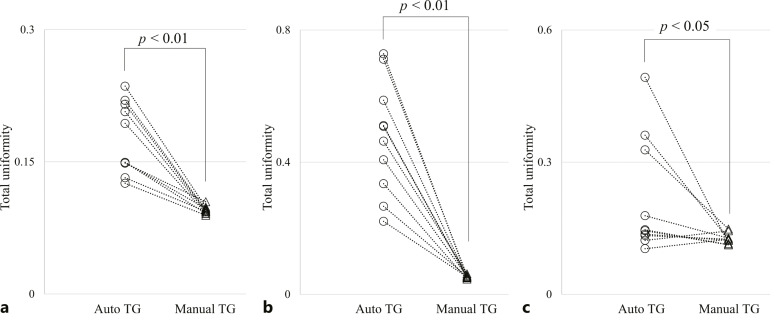
Results: The images of the phantom with the auto TG showed substantial variations between the preset and actual FAs (p < 0.01), whereas on the images with the manual TG, there were no variations between the two FAs (p > 0.05). The total image uniformity was considerably lower with the manual TG than with the auto TG (p < 0.01), indicating that the image's signal values with the manual TG were more uniform. The manual TG produced significantly higher SNRs than the auto TG (p < 0.01). In the clinical study, the lesions were clearly detected in intraoperative images with the manual TG, but they were difficult to identify in images with the auto TG. The CNR of lesions in images with manual TG was considerably higher than in images with auto TG (p < 0.01).
Conclusion: Regarding intraoperative T2WIs using a 3.0T MRI system during TcMRgFUS, the manual TG method improved image quality and delineated the ablative lesion more clearly than the current method with auto TG.
期刊介绍:
''Stereotactic and Functional Neurosurgery'' provides a single source for the reader to keep abreast of developments in the most rapidly advancing subspecialty within neurosurgery. Technological advances in computer-assisted surgery, robotics, imaging and neurophysiology are being applied to clinical problems with ever-increasing rapidity in stereotaxis more than any other field, providing opportunities for new approaches to surgical and radiotherapeutic management of diseases of the brain, spinal cord, and spine. Issues feature advances in the use of deep-brain stimulation, imaging-guided techniques in stereotactic biopsy and craniotomy, stereotactic radiosurgery, and stereotactically implanted and guided radiotherapeutics and biologicals in the treatment of functional and movement disorders, brain tumors, and other diseases of the brain. Background information from basic science laboratories related to such clinical advances provides the reader with an overall perspective of this field. Proceedings and abstracts from many of the key international meetings furnish an overview of this specialty available nowhere else. ''Stereotactic and Functional Neurosurgery'' meets the information needs of both investigators and clinicians in this rapidly advancing field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
