Carmela Martini, Jessica M Logan, Alexandra Sorvina, Sarita Prabhakaran, Benjamin S Y Ung, Ian R D Johnson, Shane M Hickey, Robert D Brooks, Maria C Caruso, Sonja Klebe, Litsa Karageorgos, John J O'Leary, Brett Delahunt, Hemamali Samaratunga, Douglas A Brooks
{"title":"Distinct patterns of biomarker expression for atypical intraductal proliferations in prostate cancer.","authors":"Carmela Martini, Jessica M Logan, Alexandra Sorvina, Sarita Prabhakaran, Benjamin S Y Ung, Ian R D Johnson, Shane M Hickey, Robert D Brooks, Maria C Caruso, Sonja Klebe, Litsa Karageorgos, John J O'Leary, Brett Delahunt, Hemamali Samaratunga, Douglas A Brooks","doi":"10.1007/s00428-023-03643-1","DOIUrl":null,"url":null,"abstract":"<p><p>High-grade prostatic intraepithelial neoplasia (HGPIN) is a well-characterised precursor lesion in prostate cancer. The term atypical intraductal proliferations (AIP) describes lesions with features that are far too atypical to be considered HGPIN, yet insufficient to be diagnosed as intraductal carcinoma of the prostate (IDCP). Here, a panel of biomarkers was assessed to provide insights into the biological relationship between IDCP, HGPIN, and AIP and their relevance to current clinicopathological recommendations. Tissue samples from 86 patients with prostate cancer were assessed by routine haematoxylin and eosin staining and immunohistochemistry (IHC) with a biomarker panel (Appl1/Sortilin/Syndecan-1) and a PIN4 cocktail (34βE12+P63/P504S). Appl1 strongly labelled atypical secretory cells, effectively visualising intraductal lesions. Sortilin labelling was moderate-to-strong in > 70% of cases, while Syndecan-1 was moderate-to-strong in micropapillary HGPIN/AIP lesions (83% cases) versus flat/tufting HGPIN (≤ 20% cases). Distinct biomarker labelling patterns for atypical intraductal lesions of the prostate were observed, including early atypical changes (flat/tufting HGPIN) and more advanced atypical changes (micropapillary HGPIN/AIP). Furthermore, the biomarker panel may be used as a tool to overcome the diagnostic uncertainty surrounding AIP by supporting a definitive diagnosis of IDCP for such lesions displaying the same biomarker pattern as cribriform IDCP.</p>","PeriodicalId":23514,"journal":{"name":"Virchows Archiv","volume":" ","pages":"723-728"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11522086/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Virchows Archiv","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00428-023-03643-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/9/14 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PATHOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
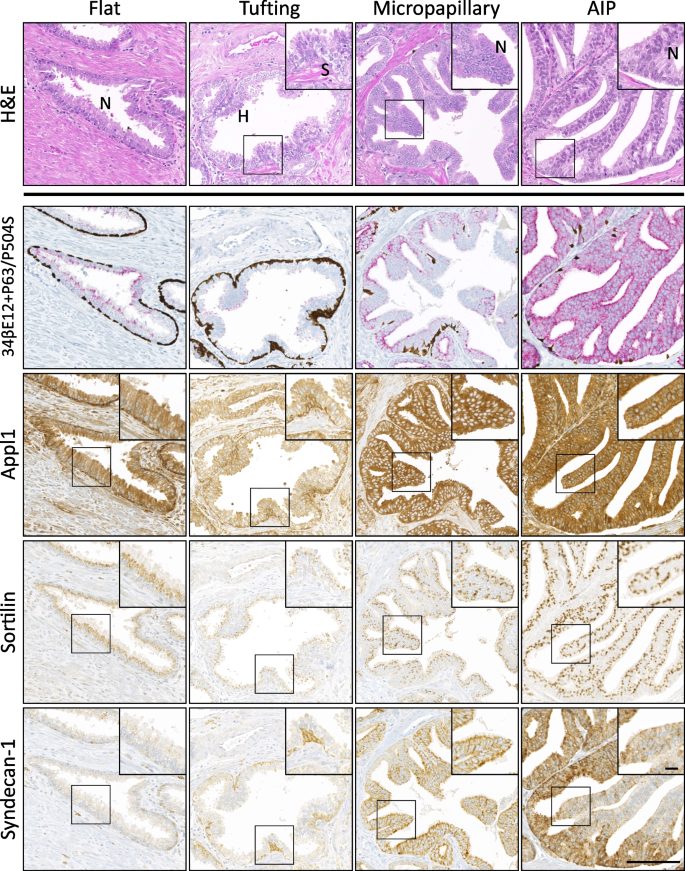
High-grade prostatic intraepithelial neoplasia (HGPIN) is a well-characterised precursor lesion in prostate cancer. The term atypical intraductal proliferations (AIP) describes lesions with features that are far too atypical to be considered HGPIN, yet insufficient to be diagnosed as intraductal carcinoma of the prostate (IDCP). Here, a panel of biomarkers was assessed to provide insights into the biological relationship between IDCP, HGPIN, and AIP and their relevance to current clinicopathological recommendations. Tissue samples from 86 patients with prostate cancer were assessed by routine haematoxylin and eosin staining and immunohistochemistry (IHC) with a biomarker panel (Appl1/Sortilin/Syndecan-1) and a PIN4 cocktail (34βE12+P63/P504S). Appl1 strongly labelled atypical secretory cells, effectively visualising intraductal lesions. Sortilin labelling was moderate-to-strong in > 70% of cases, while Syndecan-1 was moderate-to-strong in micropapillary HGPIN/AIP lesions (83% cases) versus flat/tufting HGPIN (≤ 20% cases). Distinct biomarker labelling patterns for atypical intraductal lesions of the prostate were observed, including early atypical changes (flat/tufting HGPIN) and more advanced atypical changes (micropapillary HGPIN/AIP). Furthermore, the biomarker panel may be used as a tool to overcome the diagnostic uncertainty surrounding AIP by supporting a definitive diagnosis of IDCP for such lesions displaying the same biomarker pattern as cribriform IDCP.
期刊介绍:
Manuscripts of original studies reinforcing the evidence base of modern diagnostic pathology, using immunocytochemical, molecular and ultrastructural techniques, will be welcomed. In addition, papers on critical evaluation of diagnostic criteria but also broadsheets and guidelines with a solid evidence base will be considered. Consideration will also be given to reports of work in other fields relevant to the understanding of human pathology as well as manuscripts on the application of new methods and techniques in pathology. Submission of purely experimental articles is discouraged but manuscripts on experimental work applicable to diagnostic pathology are welcomed. Biomarker studies are welcomed but need to abide by strict rules (e.g. REMARK) of adequate sample size and relevant marker choice. Single marker studies on limited patient series without validated application will as a rule not be considered. Case reports will only be considered when they provide substantial new information with an impact on understanding disease or diagnostic practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
