The Restrictive Red Blood Cell Transfusion Strategy for Critically Injured Patients (RESTRIC) trial: a cluster-randomized, crossover, non-inferiority multicenter trial of restrictive transfusion in trauma.
{"title":"The Restrictive Red Blood Cell Transfusion Strategy for Critically Injured Patients (RESTRIC) trial: a cluster-randomized, crossover, non-inferiority multicenter trial of restrictive transfusion in trauma.","authors":"Mineji Hayakawa, Takashi Tagami, Daisuke Kudo, Kota Ono, Makoto Aoki, Akira Endo, Tetsuya Yumoto, Yosuke Matsumura, Shiho Irino, Kazuhiko Sekine, Noritaka Ushio, Takayuki Ogura, Sho Nachi, Yuhei Irie, Katsura Hayakawa, Yusuke Ito, Yuko Okishio, Tomohiro Muronoi, Yoshinori Kosaki, Kaori Ito, Keita Nakatsutsumi, Yutaka Kondo, Taichiro Ueda, Hiroshi Fukuma, Yuichi Saisaka, Naoki Tominaga, Takeo Kurita, Fumihiko Nakayama, Tomotaka Shibata, Shigeki Kushimoto","doi":"10.1186/s40560-023-00682-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The efficacies of fresh frozen plasma and coagulation factor transfusion have been widely evaluated in trauma-induced coagulopathy management during the acute post-injury phase. However, the efficacy of red blood cell transfusion has not been adequately investigated in patients with severe trauma, and the optimal hemoglobin target level during the acute post-injury and resuscitation phases remains unclear. Therefore, this study aimed to examine whether a restrictive transfusion strategy was clinically non-inferior to a liberal transfusion strategy during the acute post-injury phase.</p><p><strong>Methods: </strong>This cluster-randomized, crossover, non-inferiority multicenter trial was conducted at 22 tertiary emergency medical institutions in Japan and included adult patients with severe trauma at risk of major bleeding. The institutions were allocated a restrictive or liberal transfusion strategy (target hemoglobin levels: 7-9 or 10-12 g/dL, respectively). The strategies were applied to patients immediately after arrival at the emergency department. The primary outcome was 28-day survival after arrival at the emergency department. Secondary outcomes included transfusion volume, complication rates, and event-free days. The non-inferiority margin was set at 3%.</p><p><strong>Results: </strong>The 28-day survival rates of patients in the restrictive (n = 216) and liberal (n = 195) strategy groups were 92.1% and 91.3%, respectively. The adjusted odds ratio for 28-day survival in the restrictive versus liberal strategy group was 1.02 (95% confidence interval: 0.49-2.13). Significant non-inferiority was not observed. Transfusion volumes and hemoglobin levels were lower in the restrictive strategy group than in the liberal strategy group. No between-group differences were noted in complication rates or event-free days.</p><p><strong>Conclusions: </strong>Although non-inferiority of the restrictive versus liberal transfusion strategy for 28-day survival was not statistically significant, the mortality and complication rates were similar between the groups. The restrictive transfusion strategy results in a lower transfusion volume.</p><p><strong>Trial registration number: </strong>umin.ac.jp/ctr: UMIN000034405, registration date: 8 October 2018.</p>","PeriodicalId":16123,"journal":{"name":"Journal of Intensive Care","volume":"11 1","pages":"34"},"PeriodicalIF":4.7000,"publicationDate":"2023-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10364403/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Intensive Care","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40560-023-00682-3","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The efficacies of fresh frozen plasma and coagulation factor transfusion have been widely evaluated in trauma-induced coagulopathy management during the acute post-injury phase. However, the efficacy of red blood cell transfusion has not been adequately investigated in patients with severe trauma, and the optimal hemoglobin target level during the acute post-injury and resuscitation phases remains unclear. Therefore, this study aimed to examine whether a restrictive transfusion strategy was clinically non-inferior to a liberal transfusion strategy during the acute post-injury phase.
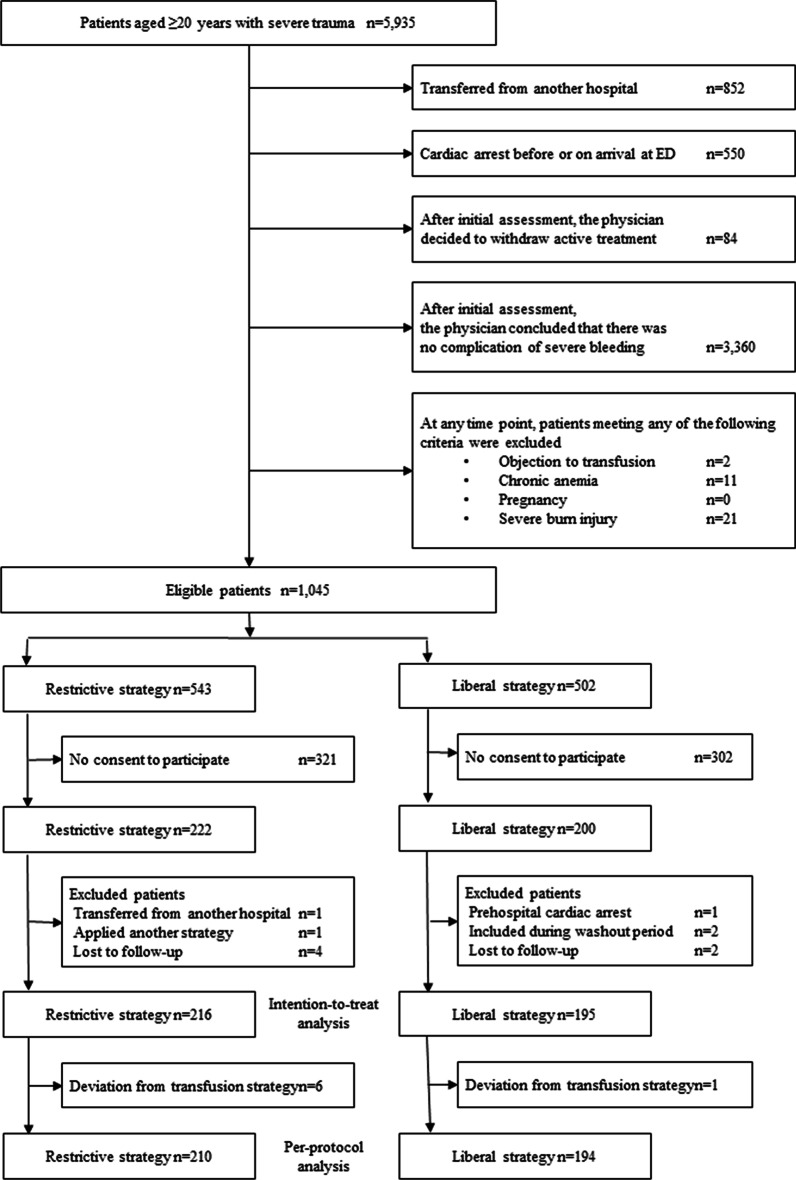
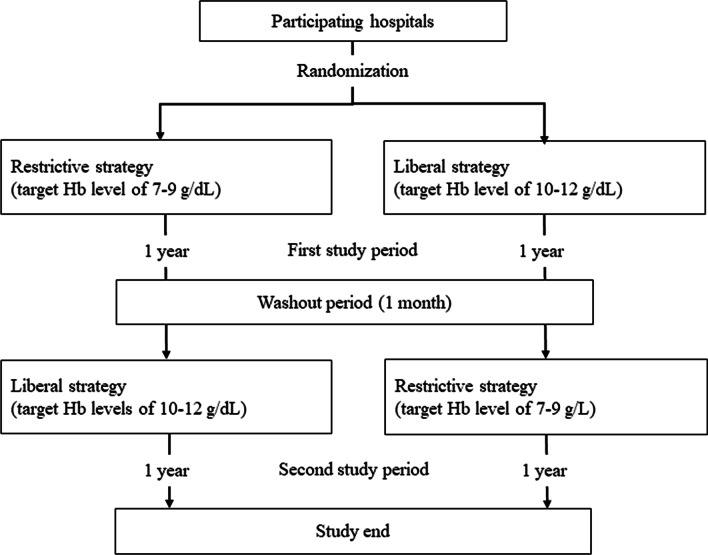
Methods: This cluster-randomized, crossover, non-inferiority multicenter trial was conducted at 22 tertiary emergency medical institutions in Japan and included adult patients with severe trauma at risk of major bleeding. The institutions were allocated a restrictive or liberal transfusion strategy (target hemoglobin levels: 7-9 or 10-12 g/dL, respectively). The strategies were applied to patients immediately after arrival at the emergency department. The primary outcome was 28-day survival after arrival at the emergency department. Secondary outcomes included transfusion volume, complication rates, and event-free days. The non-inferiority margin was set at 3%.
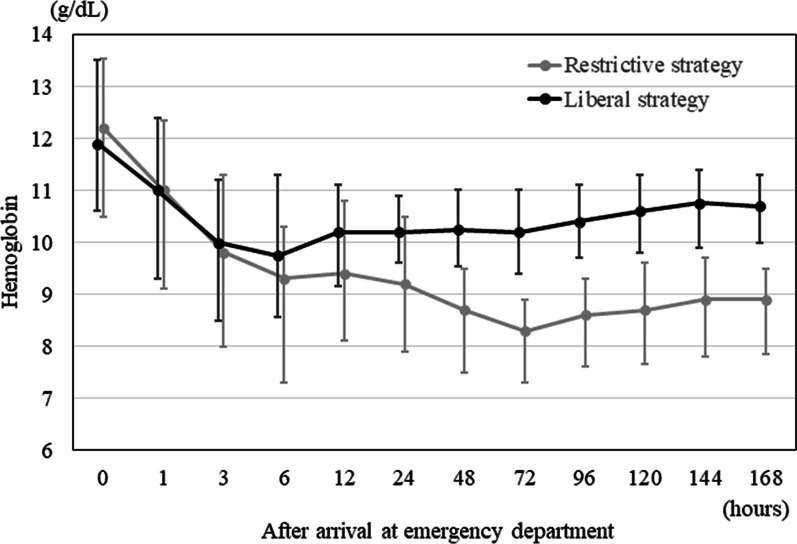
Results: The 28-day survival rates of patients in the restrictive (n = 216) and liberal (n = 195) strategy groups were 92.1% and 91.3%, respectively. The adjusted odds ratio for 28-day survival in the restrictive versus liberal strategy group was 1.02 (95% confidence interval: 0.49-2.13). Significant non-inferiority was not observed. Transfusion volumes and hemoglobin levels were lower in the restrictive strategy group than in the liberal strategy group. No between-group differences were noted in complication rates or event-free days.
Conclusions: Although non-inferiority of the restrictive versus liberal transfusion strategy for 28-day survival was not statistically significant, the mortality and complication rates were similar between the groups. The restrictive transfusion strategy results in a lower transfusion volume.
Trial registration number: umin.ac.jp/ctr: UMIN000034405, registration date: 8 October 2018.
期刊介绍:
"Journal of Intensive Care" is an open access journal dedicated to the comprehensive coverage of intensive care medicine, providing a platform for the latest research and clinical insights in this critical field. The journal covers a wide range of topics, including intensive and critical care, trauma and surgical intensive care, pediatric intensive care, acute and emergency medicine, perioperative medicine, resuscitation, infection control, and organ dysfunction.
Recognizing the importance of cultural diversity in healthcare practices, "Journal of Intensive Care" also encourages submissions that explore and discuss the cultural aspects of intensive care, aiming to promote a more inclusive and culturally sensitive approach to patient care. By fostering a global exchange of knowledge and expertise, the journal contributes to the continuous improvement of intensive care practices worldwide.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
