Marek Szamborski, Jarosław Janc, Patrycja Leśnik, Artur Milnerowicz, Dariusz Jagielski, Lidia Łysenko
{"title":"Ultrasound-Guided Pectoserratus Plane Block and Superficial Serratus Anterior Plane Block for Subcutaneous Implantable Cardioverter-Defibrillator Implantation: A Comparative Study.","authors":"Marek Szamborski, Jarosław Janc, Patrycja Leśnik, Artur Milnerowicz, Dariusz Jagielski, Lidia Łysenko","doi":"10.12659/MSM.940541","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND The combination of pectoserratus plane block (PSP) and superficial serratus anterior plane block (S-SAP) was established to reduce the risk of general anesthesia for subcutaneous implantable cardioverter-defibrillator (S-ICD) implantation in patients with high operative risk (American Society of Anesthesiologistsgrade III or IV). This study compared outcomes from ultrasound-guided PSP and S-SAP in 16 patients requiring a subcutaneous implantable cardioverter-defibrillator (S-ICD) at a single center in Poland. MATERIAL AND METHODS A group of 16 patients with ASA grade III and IV qualified for S-ICD implantation was included. The pain assessment using numerical rating scale (NRS), patient's comfort using Quality of Recovery-15 (QoR-15), the operator's satisfaction using Operator's Comfort Scale, adverse event occurrence, and the parameters' stability were evaluated. RESULTS The mean volume of the local anesthetics mixture of PSP block was 19.4 mL; S-SAP was 34.7 mL (mean total volume, 54.1 mL). The mean duration of the block was 21.3 min; the mean time of the S-ICD implantation was 108.4 min. Neither circulatory nor respiratory instability was observed. In 8 patients (50%), non-opioid analgesics were administered intraoperatively; in 11 patients (69%), fentanyl bolus ≤200 μg was administered. The intraoperative NRS score was low (max 2 points); NRS 24 h after the procedure was low (max 4 points). The mean value of QoR-15 was 133.9 points. CONCLUSIONS S-SAP combined with PSP is feasible and safe in providing anesthesia/analgesia during S-ICD implantation and showed good effects in a group of patients with high operative risk (ASA III or IV).</p>","PeriodicalId":18276,"journal":{"name":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","volume":"29 ","pages":"e940541"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e2/f6/medscimonit-29-e940541.PMC10368141.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medical Science Monitor : International Medical Journal of Experimental and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/MSM.940541","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
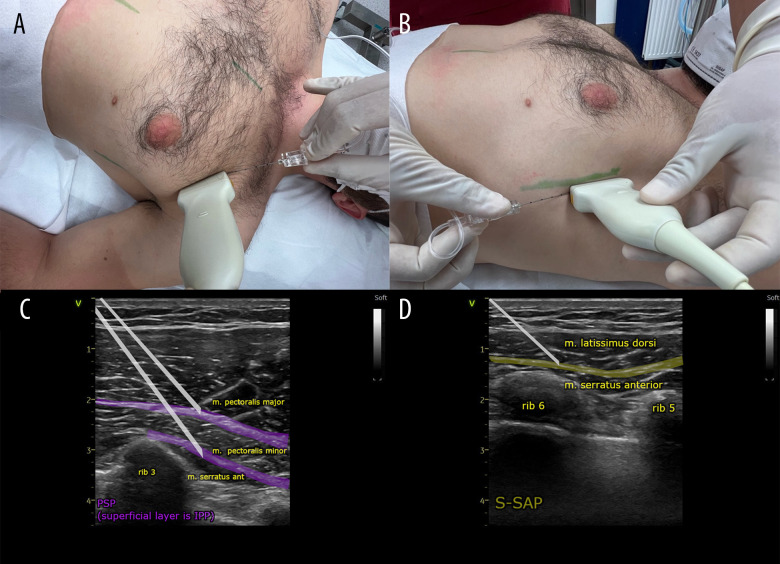
BACKGROUND The combination of pectoserratus plane block (PSP) and superficial serratus anterior plane block (S-SAP) was established to reduce the risk of general anesthesia for subcutaneous implantable cardioverter-defibrillator (S-ICD) implantation in patients with high operative risk (American Society of Anesthesiologistsgrade III or IV). This study compared outcomes from ultrasound-guided PSP and S-SAP in 16 patients requiring a subcutaneous implantable cardioverter-defibrillator (S-ICD) at a single center in Poland. MATERIAL AND METHODS A group of 16 patients with ASA grade III and IV qualified for S-ICD implantation was included. The pain assessment using numerical rating scale (NRS), patient's comfort using Quality of Recovery-15 (QoR-15), the operator's satisfaction using Operator's Comfort Scale, adverse event occurrence, and the parameters' stability were evaluated. RESULTS The mean volume of the local anesthetics mixture of PSP block was 19.4 mL; S-SAP was 34.7 mL (mean total volume, 54.1 mL). The mean duration of the block was 21.3 min; the mean time of the S-ICD implantation was 108.4 min. Neither circulatory nor respiratory instability was observed. In 8 patients (50%), non-opioid analgesics were administered intraoperatively; in 11 patients (69%), fentanyl bolus ≤200 μg was administered. The intraoperative NRS score was low (max 2 points); NRS 24 h after the procedure was low (max 4 points). The mean value of QoR-15 was 133.9 points. CONCLUSIONS S-SAP combined with PSP is feasible and safe in providing anesthesia/analgesia during S-ICD implantation and showed good effects in a group of patients with high operative risk (ASA III or IV).



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
