Yoon Hae Ahn, Hong Yeul Lee, Sang-Min Lee, Jinwoo Lee
{"title":"Factors influencing sleep quality in the intensive care unit: a descriptive pilot study in Korea.","authors":"Yoon Hae Ahn, Hong Yeul Lee, Sang-Min Lee, Jinwoo Lee","doi":"10.4266/acc.2023.00514","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>As sleep disturbances are common in the intensive care unit (ICU), this study assessed the sleep quality in the ICU and identified barriers to sleep.</p><p><strong>Methods: </strong>Patients admitted to the ICUs of a tertiary hospital between June 2022 and December 2022 who were not mechanically ventilated at enrollment were included. The quality of sleep (QoS) at home was assessed on a visual analog scale as part of an eight-item survey, while the QoS in the ICU was evaluated using the Korean version of the Richards-Campbell Sleep Questionnaire (K-RCSQ). Good QoS was defined by a score of ≥50.</p><p><strong>Results: </strong>Of the 30 patients in the study, 19 reported a QoS score <50. The Spearman correlation coefficient showed no meaningful relationship between the QoS at home and the overall K-RCSQ QoS score in the ICU (r=0.16, P=0.40). The most common barriers to sleep were physical discomfort (43%), being awoken for procedures (43%), and feeling unwell (37%); environmental factors including noise (30%) and light (13%) were also identified sources of sleep disruption. Physical discomfort (median [interquartile range]: 32 [28.0-38.0] vs. 69 [42.0-80.0], P=0.004), being awoken for procedures (36 [20.0-48.0] vs. 54 [36.0-80.0], P=0.04), and feeling unwell (31 [18.0-42.0] vs. 54 [40.0-76.0], P=0.01) were associated with lower K-RCSQ scores.</p><p><strong>Conclusions: </strong>In the ICU, physical discomfort, patient care interactions, and feeling unwell were identified as barriers to sleep.</p>","PeriodicalId":44118,"journal":{"name":"Acute and Critical Care","volume":"38 3","pages":"278-285"},"PeriodicalIF":2.0000,"publicationDate":"2023-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2a/fa/acc-2023-00514.PMC10497899.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acute and Critical Care","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4266/acc.2023.00514","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Background: As sleep disturbances are common in the intensive care unit (ICU), this study assessed the sleep quality in the ICU and identified barriers to sleep.
Methods: Patients admitted to the ICUs of a tertiary hospital between June 2022 and December 2022 who were not mechanically ventilated at enrollment were included. The quality of sleep (QoS) at home was assessed on a visual analog scale as part of an eight-item survey, while the QoS in the ICU was evaluated using the Korean version of the Richards-Campbell Sleep Questionnaire (K-RCSQ). Good QoS was defined by a score of ≥50.
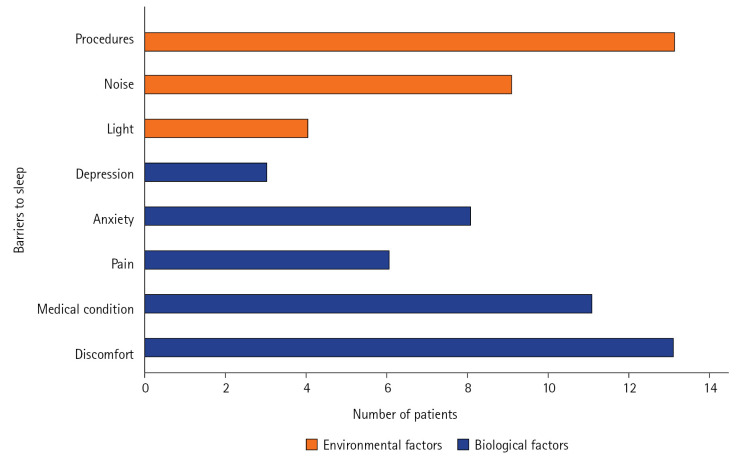
Results: Of the 30 patients in the study, 19 reported a QoS score <50. The Spearman correlation coefficient showed no meaningful relationship between the QoS at home and the overall K-RCSQ QoS score in the ICU (r=0.16, P=0.40). The most common barriers to sleep were physical discomfort (43%), being awoken for procedures (43%), and feeling unwell (37%); environmental factors including noise (30%) and light (13%) were also identified sources of sleep disruption. Physical discomfort (median [interquartile range]: 32 [28.0-38.0] vs. 69 [42.0-80.0], P=0.004), being awoken for procedures (36 [20.0-48.0] vs. 54 [36.0-80.0], P=0.04), and feeling unwell (31 [18.0-42.0] vs. 54 [40.0-76.0], P=0.01) were associated with lower K-RCSQ scores.
Conclusions: In the ICU, physical discomfort, patient care interactions, and feeling unwell were identified as barriers to sleep.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
