Julia Feige, Fritz Klausner, Johannes A. R. Pfaff, Eugen Trinka, Slaven Pikija, Mahdi Safdarian
{"title":"Stroke-like presentation of acute toxic leukoencephalopathy due to capecitabine treatment with extensive intramyelinic edema","authors":"Julia Feige, Fritz Klausner, Johannes A. R. Pfaff, Eugen Trinka, Slaven Pikija, Mahdi Safdarian","doi":"10.1002/cdt3.72","DOIUrl":null,"url":null,"abstract":"<p>Capecitabine is an oral prodrug of 5-fluorouracil (5-FU), which is widely used for adjuvant and neoadjuvant chemotherapy of different solid tumors, particularly breast and colorectal cancers.<span><sup>1</sup></span> Neurotoxicity of capecitabine has been consistently reported as capecitabine-induced toxic leukoencephalopathy, which includes bilateral lesions in the corpus callosum and corticospinal tract presenting as acute or delayed central nervous system toxicity.<span><sup>2</sup></span> This side effect requires discontinuation of chemotherapy<span><sup>3</sup></span>; however, neurological symptoms due to capecitabine are reported to be usually reversible upon drug withdrawal.<span><sup>1</sup></span></p><p>The patients presenting with acute stroke-like symptoms with accompanied restricted diffusion outside typical vessel territory pose a significant diagnostic challenge. In the case of exclusively white matter involvement, the observed low apparent diffusion coefficient (ADC) could be due to the severe intramyelinic edema and not cell death, that is, cytotoxic edema. Multifocal leukoencephalopathy has been associated with capecitabine, but only a few cases have been reported in the literature.<span><sup>4</sup></span></p><p>A 51-year-old woman was admitted due to acute onset of dizziness, dysarthria, and right-sided central facial paresis. The patient had been diagnosed with bilateral breast cancer 5 years ago for which neoadjuvant chemotherapy was done as well as surgical and radiation therapy. The primary tumor was a moderately differentiated invasive breast carcinoma of nonspecific type (right breast: stadium cT1b, human epidermal growth factor receptor 2 [HER2] negative with Ki67 10%–20%, and left breast: Stadium cT1c cN1 cM0. HER2 negative. Ki67 10%). Neoadjuvant chemotherapy regime consisted of four cycles of epirubicin/cyclophosphamide (every 2 weeks [q2w]) afterwards four cycles of paclitaxel (q2w) with granulocyte-colony-stimulating factor (G-CSF) support for 4 months. In the follow-up fluorodeoxyglucose-positron emission tomography (FDG-PET) scan, a solitary osseous metastasis was detected in the sacrum, for which capecitabine and bevacizumab had been initiated.</p><p>At our department, the patient reported a feeling of dizziness and difficulties in swallowing 1 day after starting capecitabine and bevacizumab. The CT at admission showed no infarction or hemorrhage and she was also outside thrombolysis therapeutic window. In the evening that day, there was a sudden onset of motoric aphasia. MR-tomography showed a pronounced hyperintense white matter lesion affecting the splenium of the corpus callosum and the medullary beds with pronounced fiber rarefication in arcuate fasciculus (Figure 1A–C). There was a mild pleocytosis of 15 cells/μL in the CSF, with normal protein and lactate. A JC virus polymerase chain reaction (PCR) from the CSF was negative. Onco-neural and antineuronal antibodies were all negative (Table 1). Clinical symptoms resolved rapidly 1 day after discontinuation of capecitabine. About 2 months later, a control MRI showed only discrete hyperintensity in the splenium with normal fiber-tracking (Figure 1D–F).</p><p>Upon discharge, 3 weeks radiation of solitary metastasis in S1 sacral bone with 15 × 3 Gy (cumulative 45 Gy) was done as an alternative treatment for her metastatic disease.</p><p>Here we presented a case of acute onset of motoric aphasia developed immediately after initiating capecitabine, with prompt resolution of clinical symptoms upon its discontinuation.</p><p>Capecitabine, upon oral ingestion, is activated through the triple enzymatic process (carboxylesterase, cytidine deaminase, and thymidine phosphorylase), resulting in the formation of 5-FU.<span><sup>5</sup></span> 5-FU would be preferentially produced in cancer cells due to higher levels of thymidine phosphorylase,<span><sup>6</sup></span> and undergo catabolism through dihydropyrimidine dehydrogenase (DYPD) in the liver. DYPD deficiency, therefore, leads to severe toxicity due to accumulating 5-FU. However, DYPD deficiency is nowadays a rare cause of 5-FU toxicity due to regular screening. Nevertheless, other polymorphisms of the DYPD gene, which are not regularly screened, and other genes such as thymidylate synthase (TYMS) can be responsible for increased toxicity. For example, patients homozygous for the TS 3RG allele have higher toxicity and less response to treatment compared to the nonhomozygous cohort.<span><sup>7</sup></span> The capecitabine intermediate metabolite 50-deoxy-5-fluorouridine (50-DFUR) crosses the blood-brain barrier, providing the substrate for this final step of capecitabine transformation into 5-FU locally in the brain.<span><sup>8</sup></span></p><p>The lesions seen in patients with capecitabine-induced leukoencephalopathy are mostly localized in the white matter tracts and are mostly reversible. However, the imaging is inconsistent with reports ranging from “no abnormality” to extensive white matter involvement, including infratentorial as well as supratentorial tracts.</p><p>Low ADC, as seen in our patient could point to the presence of intramyelinic edema, as suggested by de Oliveira.<span><sup>9</sup></span> It postulates the existence of nonneurotoxic edema in the virtual space of myelin layers enveloping and insulating the axons. The characteristic pattern is of truly restricted water diffusibility—imitating irreversible cytotoxic edema—however, without lasting consequences on control imaging.</p><p>Posterior reversible leukoencephalopathy syndrome (PRES) could present with similar clinical symptoms. PRES presents in patients with elevated blood pressure, disorders of consciousness, epileptic seizures (almost two-thirds of patients), and visual disturbance due to involvement of posterior cerebral regions and vasogenic edema. Focal neurological signs such as aphasia seen in our patient are present in a minority of cases (up to 15%).<span><sup>10</sup></span> It could, however, involve white matter tracts, have DWI restriction, and present bilaterally. Our patient also received therapy with bevacizumab, which indeed may induce leukoencephalopathy mostly in terms of PRES.<span><sup>11</sup></span> However, possible augmentation of capecitabine-induced callosal lesion through concomitant bevacizumab administration could not be completely ruled-out.</p><p>Marchiafava-Bignami disease results from osmotic demyelination and necrosis of the corpus callosum.<span><sup>12</sup></span> It present in patients having chronic ethanol use and vitamin B complex deficiency, both not presented in our patient. DWI would not also show any changes in the acute phase.</p><p>Reversible splenial lesion (RSL), most probably would occur due to viral infection and hypoglycemia, hypernatremia, acute alcohol poisoning, and epileptic seizures. It may also manifest between 24 h to 3 weeks after withdrawal of antiepileptic drugs.<span><sup>13</sup></span></p><p>In a retrospective study, six adult patients with solid cancers developed acute toxic leukoencephalopathies with splenial lesions following treatment with 5-FU or capecitabine within 3 days of the first treatment cycle. Brain MRI showed T2/FLAIR hyperintensities in the corpus callosum, with diffusion restriction and no contrast enhancement. Upon capecitabine discontinuiation, all patients experienced full clinical-radiological recovery after a median of 8.5 days from symptom onset.<span><sup>14</sup></span></p><p>Obadia et al. reported a 45-year-old woman treated by capecitabine for breast cancer with metastatic bone lesions, who presented with nausea, headaches, muscle cramps, dysarthria, and swallowing disorder. MRI showed bilateral and symmetric high signal intensities of deep white matter, corpus callosum, and corticospinal tracts with regression upon discontinuation.<span><sup>2</sup></span></p><p>In 2005, Videnovic et al. had reported a case series of five capecitabine-induced leukoencephalopathies in four patients with advanced breast cancer and one with pancreatic carcinoma. All patients were women between 40 and 74 years of age who developed neurologic symptoms including nausea, confusion, short-term memory loss, headaches, vertigo, ataxia, and dysarthria within 7 days of initiating capecitabine for tumor progression. Brain MRI revealed increased signals in the areas of the corpus callosum, brachium pontis, and deep periventricular matter. The splenium of the corpus callosum was primarily affected in all cases. All patients improved over a few days after capecitabine withdrawal.<span><sup>15</sup></span></p><p>Wagner-Altendorf et al. reported a patient with bilateral degeneration of the corticospinal tract and progressive spastic tetraplegia after chemotherapy with capecitabine whose symptoms substantially worsened over the following years after discontinuation of therapy and finally died from aspiration pneumonia.<span><sup>1</sup></span></p><p>Resuming capecitabine might be feasible in some cases if expected benefits outweigh the risks. Perrain et al. for example, suggested resuming capecitabine in selected cases after excluding DYPD deficiency.<span><sup>14</sup></span> Bougea et al. also reported a 50-year-old woman who presented an isolated episode of dysarthria and ataxia under capecitabine, bevacizumab, and oxaliplatin treatment due to reversible multifocal leukoencephalopathy, which did not recur after readministration of chemotherapy.<span><sup>3</sup></span> Tipples et al., however, suggest seeking an alternative chemotherapy regime even after excluding DYPD deficiency.<span><sup>4</sup></span> No MRI abnormalities were, however, found in a young patient with metastatic colorectal cancer reported by Saif, who developed clinically acute cerebellar syndrome after starting capecitabine. The patient was found to have genotype deficiencies in the TYMS gene, and improved after discontinuation of capecitabine.<span><sup>16</sup></span></p><p>A summary of recent cases has been provided in the Supporting Information Table.<span><sup>17-23</sup></span></p><p>In conclusion, capecitabine-induced leukoencephalopathy is an acute toxic phenomenon resulting from mostly reversible intramyelinic edema upon exposure to 5-FU metabolites in highly active white matter tracts that can develop within days after starting treatment. Important differential consideration is reversible splenial lesions, mostly due to epileptic seizure or drug withdrawal. Clinicians should be aware of this probable side effect as early discontinuation of treatment usually leads to a good clinical outcome. Symptoms of neurotoxicity could vary but mainly consist of ataxia, dysarthria, headache, and confusion. Any sudden neurologic status change after initiating capecitabine should be investigated with a brain MRI, which generally shows subcortical white matter changes (leukoencephalopathy) in the splenium of the corpus callosum and corticospinal tracts. Discontinuation of capecitabine would usually result in rapid recovery of both clinical and imaging abnormalities.</p><p>Slaven Pikija, Julia Feige, Fritz Klausner, and Johannes A. R. Pfaff collected the data of the case. Slaven Pikija and Mahdi Safdarian drafted the manuscript. All the authors read and confirmed the final manuscript.</p><p>The authors declare no conflict of interest.</p><p>An informed concent was signed by the patient and she agreed about reporting her case anonymously.</p>","PeriodicalId":32096,"journal":{"name":"Chronic Diseases and Translational Medicine","volume":"9 3","pages":"258-262"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/19/13/CDT3-9-258.PMC10497845.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Diseases and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cdt3.72","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Capecitabine is an oral prodrug of 5-fluorouracil (5-FU), which is widely used for adjuvant and neoadjuvant chemotherapy of different solid tumors, particularly breast and colorectal cancers.1 Neurotoxicity of capecitabine has been consistently reported as capecitabine-induced toxic leukoencephalopathy, which includes bilateral lesions in the corpus callosum and corticospinal tract presenting as acute or delayed central nervous system toxicity.2 This side effect requires discontinuation of chemotherapy3; however, neurological symptoms due to capecitabine are reported to be usually reversible upon drug withdrawal.1
The patients presenting with acute stroke-like symptoms with accompanied restricted diffusion outside typical vessel territory pose a significant diagnostic challenge. In the case of exclusively white matter involvement, the observed low apparent diffusion coefficient (ADC) could be due to the severe intramyelinic edema and not cell death, that is, cytotoxic edema. Multifocal leukoencephalopathy has been associated with capecitabine, but only a few cases have been reported in the literature.4
A 51-year-old woman was admitted due to acute onset of dizziness, dysarthria, and right-sided central facial paresis. The patient had been diagnosed with bilateral breast cancer 5 years ago for which neoadjuvant chemotherapy was done as well as surgical and radiation therapy. The primary tumor was a moderately differentiated invasive breast carcinoma of nonspecific type (right breast: stadium cT1b, human epidermal growth factor receptor 2 [HER2] negative with Ki67 10%–20%, and left breast: Stadium cT1c cN1 cM0. HER2 negative. Ki67 10%). Neoadjuvant chemotherapy regime consisted of four cycles of epirubicin/cyclophosphamide (every 2 weeks [q2w]) afterwards four cycles of paclitaxel (q2w) with granulocyte-colony-stimulating factor (G-CSF) support for 4 months. In the follow-up fluorodeoxyglucose-positron emission tomography (FDG-PET) scan, a solitary osseous metastasis was detected in the sacrum, for which capecitabine and bevacizumab had been initiated.
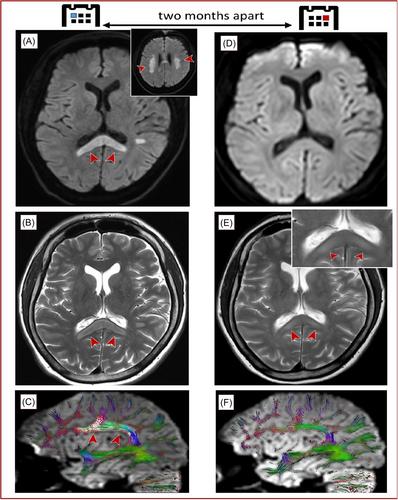
At our department, the patient reported a feeling of dizziness and difficulties in swallowing 1 day after starting capecitabine and bevacizumab. The CT at admission showed no infarction or hemorrhage and she was also outside thrombolysis therapeutic window. In the evening that day, there was a sudden onset of motoric aphasia. MR-tomography showed a pronounced hyperintense white matter lesion affecting the splenium of the corpus callosum and the medullary beds with pronounced fiber rarefication in arcuate fasciculus (Figure 1A–C). There was a mild pleocytosis of 15 cells/μL in the CSF, with normal protein and lactate. A JC virus polymerase chain reaction (PCR) from the CSF was negative. Onco-neural and antineuronal antibodies were all negative (Table 1). Clinical symptoms resolved rapidly 1 day after discontinuation of capecitabine. About 2 months later, a control MRI showed only discrete hyperintensity in the splenium with normal fiber-tracking (Figure 1D–F).
Upon discharge, 3 weeks radiation of solitary metastasis in S1 sacral bone with 15 × 3 Gy (cumulative 45 Gy) was done as an alternative treatment for her metastatic disease.
Here we presented a case of acute onset of motoric aphasia developed immediately after initiating capecitabine, with prompt resolution of clinical symptoms upon its discontinuation.
Capecitabine, upon oral ingestion, is activated through the triple enzymatic process (carboxylesterase, cytidine deaminase, and thymidine phosphorylase), resulting in the formation of 5-FU.5 5-FU would be preferentially produced in cancer cells due to higher levels of thymidine phosphorylase,6 and undergo catabolism through dihydropyrimidine dehydrogenase (DYPD) in the liver. DYPD deficiency, therefore, leads to severe toxicity due to accumulating 5-FU. However, DYPD deficiency is nowadays a rare cause of 5-FU toxicity due to regular screening. Nevertheless, other polymorphisms of the DYPD gene, which are not regularly screened, and other genes such as thymidylate synthase (TYMS) can be responsible for increased toxicity. For example, patients homozygous for the TS 3RG allele have higher toxicity and less response to treatment compared to the nonhomozygous cohort.7 The capecitabine intermediate metabolite 50-deoxy-5-fluorouridine (50-DFUR) crosses the blood-brain barrier, providing the substrate for this final step of capecitabine transformation into 5-FU locally in the brain.8
The lesions seen in patients with capecitabine-induced leukoencephalopathy are mostly localized in the white matter tracts and are mostly reversible. However, the imaging is inconsistent with reports ranging from “no abnormality” to extensive white matter involvement, including infratentorial as well as supratentorial tracts.
Low ADC, as seen in our patient could point to the presence of intramyelinic edema, as suggested by de Oliveira.9 It postulates the existence of nonneurotoxic edema in the virtual space of myelin layers enveloping and insulating the axons. The characteristic pattern is of truly restricted water diffusibility—imitating irreversible cytotoxic edema—however, without lasting consequences on control imaging.
Posterior reversible leukoencephalopathy syndrome (PRES) could present with similar clinical symptoms. PRES presents in patients with elevated blood pressure, disorders of consciousness, epileptic seizures (almost two-thirds of patients), and visual disturbance due to involvement of posterior cerebral regions and vasogenic edema. Focal neurological signs such as aphasia seen in our patient are present in a minority of cases (up to 15%).10 It could, however, involve white matter tracts, have DWI restriction, and present bilaterally. Our patient also received therapy with bevacizumab, which indeed may induce leukoencephalopathy mostly in terms of PRES.11 However, possible augmentation of capecitabine-induced callosal lesion through concomitant bevacizumab administration could not be completely ruled-out.
Marchiafava-Bignami disease results from osmotic demyelination and necrosis of the corpus callosum.12 It present in patients having chronic ethanol use and vitamin B complex deficiency, both not presented in our patient. DWI would not also show any changes in the acute phase.
Reversible splenial lesion (RSL), most probably would occur due to viral infection and hypoglycemia, hypernatremia, acute alcohol poisoning, and epileptic seizures. It may also manifest between 24 h to 3 weeks after withdrawal of antiepileptic drugs.13
In a retrospective study, six adult patients with solid cancers developed acute toxic leukoencephalopathies with splenial lesions following treatment with 5-FU or capecitabine within 3 days of the first treatment cycle. Brain MRI showed T2/FLAIR hyperintensities in the corpus callosum, with diffusion restriction and no contrast enhancement. Upon capecitabine discontinuiation, all patients experienced full clinical-radiological recovery after a median of 8.5 days from symptom onset.14
Obadia et al. reported a 45-year-old woman treated by capecitabine for breast cancer with metastatic bone lesions, who presented with nausea, headaches, muscle cramps, dysarthria, and swallowing disorder. MRI showed bilateral and symmetric high signal intensities of deep white matter, corpus callosum, and corticospinal tracts with regression upon discontinuation.2
In 2005, Videnovic et al. had reported a case series of five capecitabine-induced leukoencephalopathies in four patients with advanced breast cancer and one with pancreatic carcinoma. All patients were women between 40 and 74 years of age who developed neurologic symptoms including nausea, confusion, short-term memory loss, headaches, vertigo, ataxia, and dysarthria within 7 days of initiating capecitabine for tumor progression. Brain MRI revealed increased signals in the areas of the corpus callosum, brachium pontis, and deep periventricular matter. The splenium of the corpus callosum was primarily affected in all cases. All patients improved over a few days after capecitabine withdrawal.15
Wagner-Altendorf et al. reported a patient with bilateral degeneration of the corticospinal tract and progressive spastic tetraplegia after chemotherapy with capecitabine whose symptoms substantially worsened over the following years after discontinuation of therapy and finally died from aspiration pneumonia.1
Resuming capecitabine might be feasible in some cases if expected benefits outweigh the risks. Perrain et al. for example, suggested resuming capecitabine in selected cases after excluding DYPD deficiency.14 Bougea et al. also reported a 50-year-old woman who presented an isolated episode of dysarthria and ataxia under capecitabine, bevacizumab, and oxaliplatin treatment due to reversible multifocal leukoencephalopathy, which did not recur after readministration of chemotherapy.3 Tipples et al., however, suggest seeking an alternative chemotherapy regime even after excluding DYPD deficiency.4 No MRI abnormalities were, however, found in a young patient with metastatic colorectal cancer reported by Saif, who developed clinically acute cerebellar syndrome after starting capecitabine. The patient was found to have genotype deficiencies in the TYMS gene, and improved after discontinuation of capecitabine.16
A summary of recent cases has been provided in the Supporting Information Table.17-23
In conclusion, capecitabine-induced leukoencephalopathy is an acute toxic phenomenon resulting from mostly reversible intramyelinic edema upon exposure to 5-FU metabolites in highly active white matter tracts that can develop within days after starting treatment. Important differential consideration is reversible splenial lesions, mostly due to epileptic seizure or drug withdrawal. Clinicians should be aware of this probable side effect as early discontinuation of treatment usually leads to a good clinical outcome. Symptoms of neurotoxicity could vary but mainly consist of ataxia, dysarthria, headache, and confusion. Any sudden neurologic status change after initiating capecitabine should be investigated with a brain MRI, which generally shows subcortical white matter changes (leukoencephalopathy) in the splenium of the corpus callosum and corticospinal tracts. Discontinuation of capecitabine would usually result in rapid recovery of both clinical and imaging abnormalities.
Slaven Pikija, Julia Feige, Fritz Klausner, and Johannes A. R. Pfaff collected the data of the case. Slaven Pikija and Mahdi Safdarian drafted the manuscript. All the authors read and confirmed the final manuscript.
The authors declare no conflict of interest.
An informed concent was signed by the patient and she agreed about reporting her case anonymously.
期刊介绍:
This journal aims to promote progress from basic research to clinical practice and to provide a forum for communication among basic, translational, and clinical research practitioners and physicians from all relevant disciplines. Chronic diseases such as cardiovascular diseases, cancer, diabetes, stroke, chronic respiratory diseases (such as asthma and COPD), chronic kidney diseases, and related translational research. Topics of interest for Chronic Diseases and Translational Medicine include Research and commentary on models of chronic diseases with significant implications for disease diagnosis and treatment Investigative studies of human biology with an emphasis on disease Perspectives and reviews on research topics that discuss the implications of findings from the viewpoints of basic science and clinical practic.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
