Jeana M Holt, AkkeNeel Talsma, Teresa S Johnson, Timothy Ehlinger
{"title":"Artificial neural network approaches to identify maternal and infant risk and asset factors using Peridata.Net: a WI-MIOS study.","authors":"Jeana M Holt, AkkeNeel Talsma, Teresa S Johnson, Timothy Ehlinger","doi":"10.1093/jamiaopen/ooad080","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To analyze PeriData.Net, a clinical registry with linked maternal-infant hospital data of Milwaukee County residents, to demonstrate a predictive analytic approach to perinatal infant risk assessment.</p><p><strong>Materials and methods: </strong>Using unsupervised learning, we identified infant birth clusters with similar multivariate health indicator patterns, measured using perinatal variables from 2008 to 2019 from <i>n</i> = 43 969 clinical registry records in Milwaukee County, WI, followed by supervised learning risk-propagation modeling to identify key maternal factors. To understand the relationship between socioeconomic status (SES) and birth outcome cluster assignment, we recoded zip codes in Peridata.Net according to SES level.</p><p><strong>Results: </strong>Three self-organizing map clusters describe infant birth outcome patterns that are similar in the multivariate space. Birth outcome clusters showed higher hazard birth outcome patterns in cluster 3 than clusters 1 and 2. Cluster 3 was associated with lower Apgar scores at 1 and 5 min after birth, shorter infant length, and premature birth. Prediction profiles of birth clusters indicate the most sensitivity to pregnancy weight loss and prenatal visits. Majority of infants assigned to cluster 3 were in the 2 lowest SES levels.</p><p><strong>Discussion: </strong>Using an extensive perinatal clinical registry, we found that the strongest predictive performance, when considering cluster membership using supervised learning, was achieved by incorporating social and behavioral risk factors. There were inequalities in infant birth outcomes based on SES.</p><p><strong>Conclusion: </strong>Identifying infant risk hazard profiles can contribute to knowledge discovery and guide future research directions. Additionally, presenting the results to community members can build consensus for community-identified health and risk indicator prioritization for intervention development.</p>","PeriodicalId":36278,"journal":{"name":"JAMIA Open","volume":"6 3","pages":"ooad080"},"PeriodicalIF":3.4000,"publicationDate":"2023-09-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/97/3c/ooad080.PMC10500218.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMIA Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jamiaopen/ooad080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/10/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To analyze PeriData.Net, a clinical registry with linked maternal-infant hospital data of Milwaukee County residents, to demonstrate a predictive analytic approach to perinatal infant risk assessment.
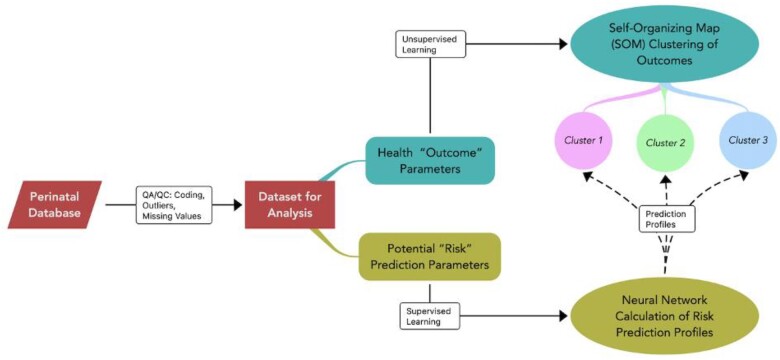
Materials and methods: Using unsupervised learning, we identified infant birth clusters with similar multivariate health indicator patterns, measured using perinatal variables from 2008 to 2019 from n = 43 969 clinical registry records in Milwaukee County, WI, followed by supervised learning risk-propagation modeling to identify key maternal factors. To understand the relationship between socioeconomic status (SES) and birth outcome cluster assignment, we recoded zip codes in Peridata.Net according to SES level.
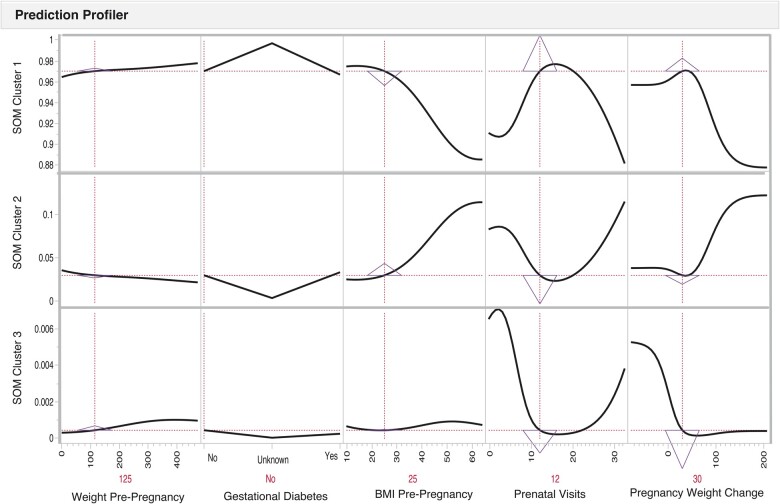
Results: Three self-organizing map clusters describe infant birth outcome patterns that are similar in the multivariate space. Birth outcome clusters showed higher hazard birth outcome patterns in cluster 3 than clusters 1 and 2. Cluster 3 was associated with lower Apgar scores at 1 and 5 min after birth, shorter infant length, and premature birth. Prediction profiles of birth clusters indicate the most sensitivity to pregnancy weight loss and prenatal visits. Majority of infants assigned to cluster 3 were in the 2 lowest SES levels.
Discussion: Using an extensive perinatal clinical registry, we found that the strongest predictive performance, when considering cluster membership using supervised learning, was achieved by incorporating social and behavioral risk factors. There were inequalities in infant birth outcomes based on SES.
Conclusion: Identifying infant risk hazard profiles can contribute to knowledge discovery and guide future research directions. Additionally, presenting the results to community members can build consensus for community-identified health and risk indicator prioritization for intervention development.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
