{"title":"Can You Establish the Cause of This Patient's Shortness of Breath?","authors":"Allison Trail, Jane Rogers, Jaffer Ajani","doi":"10.6004/jadpro.2023.14.5.8","DOIUrl":null,"url":null,"abstract":"<p><p>Mr. B is a 56-year-old man diagnosed with metastatic HER2-positive gastroesophageal adenocarcinoma. He received front-line leucovorin, 5-fluorouracil, and oxaliplatin (FOLFOX) and trastuzumab for 10 months before restaging imaging revealed progressive disease. He then received second-line trastuzumab deruxtecan. His treatment was complicated by several admissions felt to be unrelated to his cancer therapy. He was discharged after an episode of pneumonia on a steroid taper with prophylactic trimethoprim/sulfamethoxazole. Once he recovered, he was given a fourth dose of chemotherapy. About a week later, wheezes were noticed on physical exam, and he was given a 5-day course of levofloxacin. Around the same time, he also finished his steroid taper. Twelve days after his dose of chemotherapy, he presented to the emergency room with 3 to 4 days of progressive shortness of breath and dry cough following the completion of levofloxacin without symptom improvement. A CT scan showed increasing airspace opacities and multifocal areas of consolidation. Blood, nasal, and sputum cultures were negative. A bronchoscopy was performed that did not reveal findings concerning for capillaritis. He was ultimately diagnosed with drug-induced pneumonitis/interstitial lung disease (ILD). Mr. B continued to experience worsening hypoxic respiratory failure despite continuous IV steroids. He was discharged to an inpatient hospice facility where he passed away 2 weeks later. Drug-induced pneumonitis/ILD should be considered in all patients receiving trastuzumab deruxtecan who develop progressive shortness of breath or other respiratory complaints.</p>","PeriodicalId":17176,"journal":{"name":"Journal of the Advanced Practitioner in Oncology","volume":"14 5","pages":"440-443"},"PeriodicalIF":0.0000,"publicationDate":"2023-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/27/40/jadpro-14-440.PMC10414527.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Advanced Practitioner in Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.6004/jadpro.2023.14.5.8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
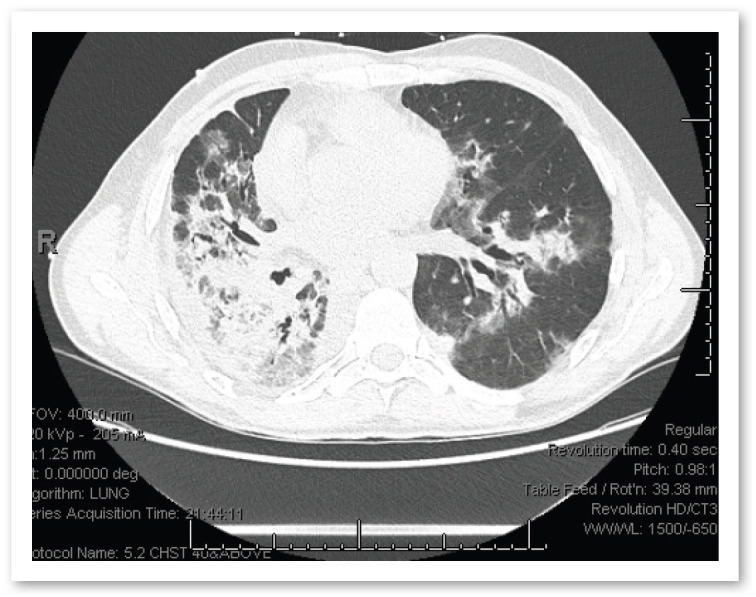
Mr. B is a 56-year-old man diagnosed with metastatic HER2-positive gastroesophageal adenocarcinoma. He received front-line leucovorin, 5-fluorouracil, and oxaliplatin (FOLFOX) and trastuzumab for 10 months before restaging imaging revealed progressive disease. He then received second-line trastuzumab deruxtecan. His treatment was complicated by several admissions felt to be unrelated to his cancer therapy. He was discharged after an episode of pneumonia on a steroid taper with prophylactic trimethoprim/sulfamethoxazole. Once he recovered, he was given a fourth dose of chemotherapy. About a week later, wheezes were noticed on physical exam, and he was given a 5-day course of levofloxacin. Around the same time, he also finished his steroid taper. Twelve days after his dose of chemotherapy, he presented to the emergency room with 3 to 4 days of progressive shortness of breath and dry cough following the completion of levofloxacin without symptom improvement. A CT scan showed increasing airspace opacities and multifocal areas of consolidation. Blood, nasal, and sputum cultures were negative. A bronchoscopy was performed that did not reveal findings concerning for capillaritis. He was ultimately diagnosed with drug-induced pneumonitis/interstitial lung disease (ILD). Mr. B continued to experience worsening hypoxic respiratory failure despite continuous IV steroids. He was discharged to an inpatient hospice facility where he passed away 2 weeks later. Drug-induced pneumonitis/ILD should be considered in all patients receiving trastuzumab deruxtecan who develop progressive shortness of breath or other respiratory complaints.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
