Elisabete Monteiro, António Ferreira, Edite Raquel Mendes, Sofia Rocha E Silva, Isabel Maia, Cláudia Camila Dias, Marek Czosnyka, José Artur Paiva, Celeste Dias
{"title":"Neurocritical care management supported by multimodal brain monitoring after acute brain injury.","authors":"Elisabete Monteiro, António Ferreira, Edite Raquel Mendes, Sofia Rocha E Silva, Isabel Maia, Cláudia Camila Dias, Marek Czosnyka, José Artur Paiva, Celeste Dias","doi":"10.5935/2965-2774.20230036-en","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the association between different intensive care units and levels of brain monitoring with outcomes in acute brain injury.</p><p><strong>Methods: </strong>Patients with traumatic brain injury and subarachnoid hemorrhage admitted to intensive care units were included. Neurocritical care unit management was compared to general intensive care unit management. Patients managed with multimodal brain monitoring and optimal cerebral perfusion pressure were compared with general management patients. A good outcome was defined as a Glasgow outcome scale score of 4 or 5.</p><p><strong>Results: </strong>Among 389 patients, 237 were admitted to the neurocritical care unit, and 152 were admitted to the general intensive care unit. Neurocritical care unit management patients had a lower risk of poor outcome (OR = 0.228). A subgroup of 69 patients with multimodal brain monitoring (G1) was compared with the remaining patients (G2). In the G1 and G2 groups, 59% versus 23% of patients, respectively, had a good outcome at intensive care unit discharge; 64% versus 31% had a good outcome at 28 days; 76% versus 50% had a good outcome at 3 months (p < 0.001); and 77% versus 58% had a good outcome at 6 months (p = 0.005). When outcomes were adjusted by SAPS II severity score, using good outcome as the dependent variable, the results were as follows: for G1 compared to G2, the OR was 4.607 at intensive care unit discharge (p < 0.001), 4.22 at 28 days (p = 0.001), 3.250 at 3 months (p = 0.001) and 2.529 at 6 months (p = 0.006). Patients with optimal cerebral perfusion pressure management (n = 127) had a better outcome at all points of evaluation. Mortality for those patients was significantly lower at 28 days (p = 0.001), 3 months (p < 0.001) and 6 months (p = 0.001).</p><p><strong>Conclusion: </strong>Multimodal brain monitoring with autoregulation and neurocritical care unit management were associated with better outcomes and should be considered after severe acute brain injury.</p>","PeriodicalId":72721,"journal":{"name":"Critical care science","volume":"35 2","pages":"196-202"},"PeriodicalIF":0.0000,"publicationDate":"2023-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10406405/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5935/2965-2774.20230036-en","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To evaluate the association between different intensive care units and levels of brain monitoring with outcomes in acute brain injury.
Methods: Patients with traumatic brain injury and subarachnoid hemorrhage admitted to intensive care units were included. Neurocritical care unit management was compared to general intensive care unit management. Patients managed with multimodal brain monitoring and optimal cerebral perfusion pressure were compared with general management patients. A good outcome was defined as a Glasgow outcome scale score of 4 or 5.
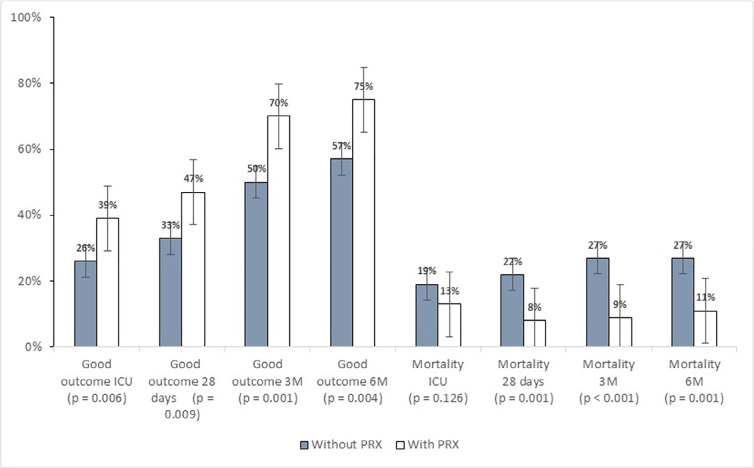
Results: Among 389 patients, 237 were admitted to the neurocritical care unit, and 152 were admitted to the general intensive care unit. Neurocritical care unit management patients had a lower risk of poor outcome (OR = 0.228). A subgroup of 69 patients with multimodal brain monitoring (G1) was compared with the remaining patients (G2). In the G1 and G2 groups, 59% versus 23% of patients, respectively, had a good outcome at intensive care unit discharge; 64% versus 31% had a good outcome at 28 days; 76% versus 50% had a good outcome at 3 months (p < 0.001); and 77% versus 58% had a good outcome at 6 months (p = 0.005). When outcomes were adjusted by SAPS II severity score, using good outcome as the dependent variable, the results were as follows: for G1 compared to G2, the OR was 4.607 at intensive care unit discharge (p < 0.001), 4.22 at 28 days (p = 0.001), 3.250 at 3 months (p = 0.001) and 2.529 at 6 months (p = 0.006). Patients with optimal cerebral perfusion pressure management (n = 127) had a better outcome at all points of evaluation. Mortality for those patients was significantly lower at 28 days (p = 0.001), 3 months (p < 0.001) and 6 months (p = 0.001).
Conclusion: Multimodal brain monitoring with autoregulation and neurocritical care unit management were associated with better outcomes and should be considered after severe acute brain injury.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
