Mingwei Sun, Qing Zong, Li Fen Ye, Yong Fan, Lijun Yang, Ru Lin
{"title":"Prognostic factors in children with acute fulminant myocarditis receiving venoarterial extracorporeal membrane oxygenation.","authors":"Mingwei Sun, Qing Zong, Li Fen Ye, Yong Fan, Lijun Yang, Ru Lin","doi":"10.1136/wjps-2021-000271","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pediatric acute fulminant myocarditis (AFM) is a very dangerous disease that may lead to acute heart failure or even sudden death. Previous reports have identified some prognostic factors in adult AFM; however, there is no such research on children with AFM on venoarterial extracorporeal membrane oxygenation (VA-ECMO). This study aimed to find relevant prognostic factors for predicting adverse clinical outcomes.</p><p><strong>Methods: </strong>A retrospective analysis was performed in an affiliated university children's hospital with consecutive patients receiving VA-ECMO for AFM from July 2010 to November 2020. These children were classified into a survivor group (n=33) and a non-survivor group (n=8). Patient demographics, clinical events, laboratory findings, and electrocardiographic and echocardiographic parameters were analyzed.</p><p><strong>Results: </strong>Peak serum creatinine (SCr) and peak creatine kinase isoenzyme MB during ECMO had joint predictive value for in-hospital mortality (p=0.011, AUC=0.962). Based on multivariable logistic regression analysis, peak SCr level during ECMO support was an independent predictor of in-hospital mortality (OR=1.035, 95% CI 1.006 to 1.064, p=0.017, AUC=0.936, with optimal cut-off value of 78 μmol/L).</p><p><strong>Conclusion: </strong>Tissue hypoperfusion and consequent end-organ damage ultimately hampered the outcomes. The need for left atrial decompression indicated a sicker patient on ECMO and introduced additional risk for complications. Earlier and more cautious deployment would likely be associated with decreased risk of complications and mortality.</p>","PeriodicalId":23823,"journal":{"name":"World Journal of Pediatric Surgery","volume":"5 1","pages":"e000271"},"PeriodicalIF":1.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/03/b2/wjps-2021-000271.PMC9717374.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/wjps-2021-000271","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Pediatric acute fulminant myocarditis (AFM) is a very dangerous disease that may lead to acute heart failure or even sudden death. Previous reports have identified some prognostic factors in adult AFM; however, there is no such research on children with AFM on venoarterial extracorporeal membrane oxygenation (VA-ECMO). This study aimed to find relevant prognostic factors for predicting adverse clinical outcomes.
Methods: A retrospective analysis was performed in an affiliated university children's hospital with consecutive patients receiving VA-ECMO for AFM from July 2010 to November 2020. These children were classified into a survivor group (n=33) and a non-survivor group (n=8). Patient demographics, clinical events, laboratory findings, and electrocardiographic and echocardiographic parameters were analyzed.
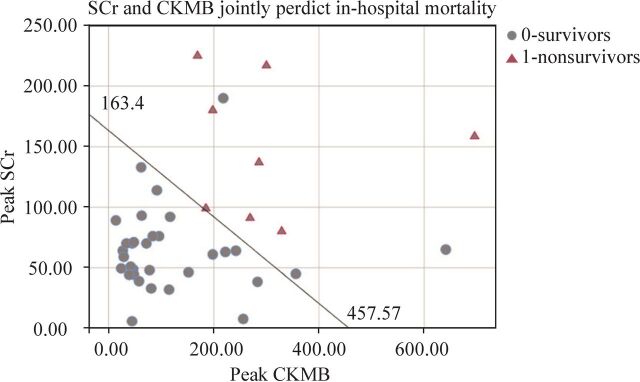
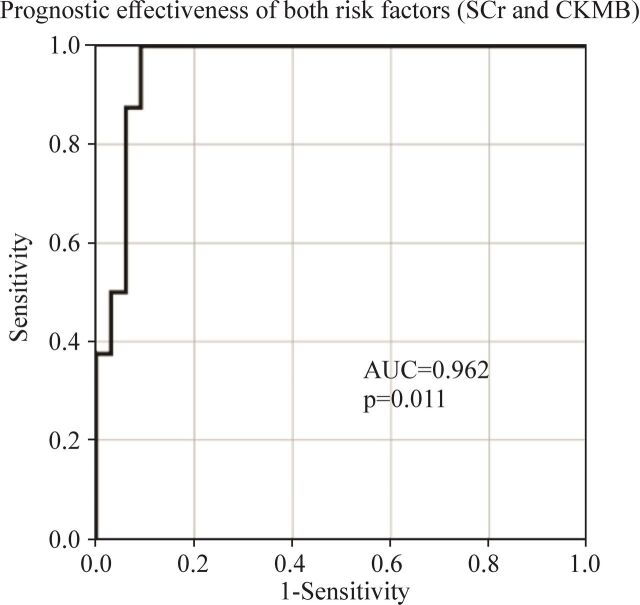
Results: Peak serum creatinine (SCr) and peak creatine kinase isoenzyme MB during ECMO had joint predictive value for in-hospital mortality (p=0.011, AUC=0.962). Based on multivariable logistic regression analysis, peak SCr level during ECMO support was an independent predictor of in-hospital mortality (OR=1.035, 95% CI 1.006 to 1.064, p=0.017, AUC=0.936, with optimal cut-off value of 78 μmol/L).
Conclusion: Tissue hypoperfusion and consequent end-organ damage ultimately hampered the outcomes. The need for left atrial decompression indicated a sicker patient on ECMO and introduced additional risk for complications. Earlier and more cautious deployment would likely be associated with decreased risk of complications and mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
