{"title":"Disorders of Movement due to Acquired and Traumatic Brain Injury.","authors":"Daniel Moon","doi":"10.1007/s40141-022-00368-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Both traumatic and acquired brain injury can result in diffuse multifocal injury affecting both the pyramidal and extrapyramidal tracts. Thus, these patients may exhibit signs of both upper motor neuron syndrome and movement disorder simultaneously which can further complicate diagnosis and management. We will be discussing movement disorders following acquired and traumatic brain injury.</p><p><strong>Recent findings: </strong>Multiple functions including speech, swallowing, posture, mobility, and activities of daily living can all be affected. Medical treatment and rehabilitation-based therapy can be especially challenging due to accompanying cognitive deficits and severity of the disorder which can involve multiple limbs in addition to muscles of the face and axial skeleton. Tremor and dystonia are the most reported movement disorders following traumatic brain injury. Dystonia and myoclonus are well documented following hypoxic ischemic brain injuries. Electrophysiological studies such as dynamic surface poly-electromyography can assist with identifying phenomenology, especially differentiating between jerk-like phenomenon and help guide further work up and management. Management with medications remains challenging due to potential adverse effects. Surgical interventions including stereotactic surgery, deep brain stimulation, and intrathecal baclofen pumps have been reported, but most of the evidence supporting them has been limited to primarily case reports except for post-traumatic tremor.</p><p><strong>Summary: </strong>Brain injury can lead to motor disorders, movement disorders, visual (processing) deficits, and vestibular deficits which often coexist with cognitive deficits making it challenging to treat and rehabilitate these patients. Unfortunately, the evidence regarding the medical management and rehabilitation of brain injury patients with movement disorders is sparse and leaves much to be desired.</p>","PeriodicalId":36406,"journal":{"name":"Current Physical Medicine and Rehabilitation Reports","volume":"10 4","pages":"311-323"},"PeriodicalIF":1.2000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9493170/pdf/","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Physical Medicine and Rehabilitation Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40141-022-00368-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"REHABILITATION","Score":null,"Total":0}
引用次数: 5
Abstract
Purpose of review: Both traumatic and acquired brain injury can result in diffuse multifocal injury affecting both the pyramidal and extrapyramidal tracts. Thus, these patients may exhibit signs of both upper motor neuron syndrome and movement disorder simultaneously which can further complicate diagnosis and management. We will be discussing movement disorders following acquired and traumatic brain injury.
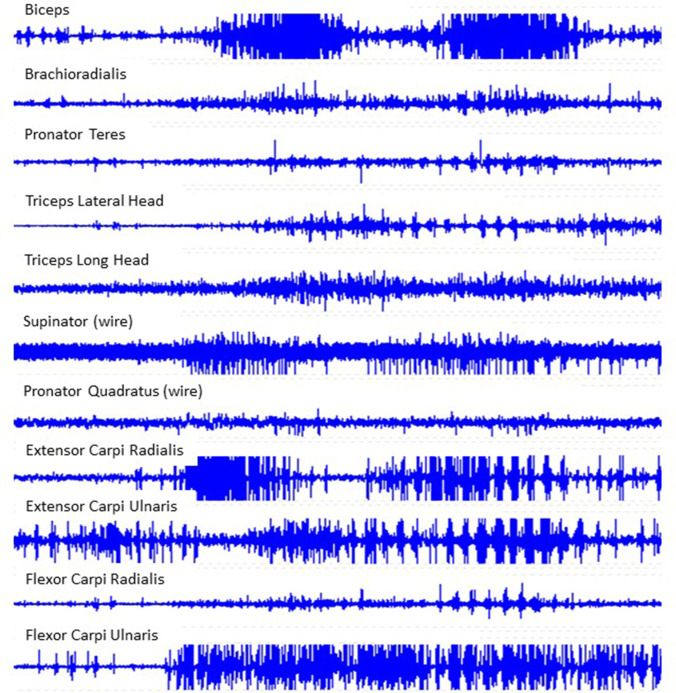
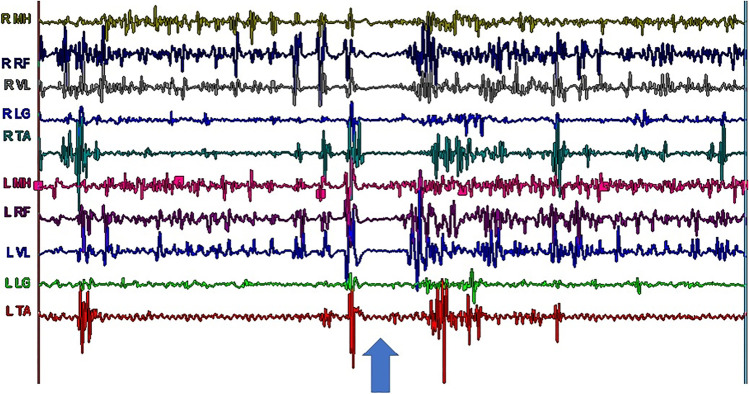
Recent findings: Multiple functions including speech, swallowing, posture, mobility, and activities of daily living can all be affected. Medical treatment and rehabilitation-based therapy can be especially challenging due to accompanying cognitive deficits and severity of the disorder which can involve multiple limbs in addition to muscles of the face and axial skeleton. Tremor and dystonia are the most reported movement disorders following traumatic brain injury. Dystonia and myoclonus are well documented following hypoxic ischemic brain injuries. Electrophysiological studies such as dynamic surface poly-electromyography can assist with identifying phenomenology, especially differentiating between jerk-like phenomenon and help guide further work up and management. Management with medications remains challenging due to potential adverse effects. Surgical interventions including stereotactic surgery, deep brain stimulation, and intrathecal baclofen pumps have been reported, but most of the evidence supporting them has been limited to primarily case reports except for post-traumatic tremor.
Summary: Brain injury can lead to motor disorders, movement disorders, visual (processing) deficits, and vestibular deficits which often coexist with cognitive deficits making it challenging to treat and rehabilitate these patients. Unfortunately, the evidence regarding the medical management and rehabilitation of brain injury patients with movement disorders is sparse and leaves much to be desired.
期刊介绍:
This journal aims to offer expert review articles on the most significant recent developments in physical medicine and rehabilitation. By providing clear, insightful, balanced contributions, the journal serves those for whom an understanding of emerging knowledge in the rehabilitation sciences is essential to optimizing health, function, and participation in individuals with physical disabilities. We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas across the field. Section Editors select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An Editorial Board of more than 20 internationally diverse members reviews the annual table of contents, ensures that topics include emerging research, and suggests topics of special importance to their country/region. Topics covered may include amputee rehabilitation; interventional pain management; musculoskeletal rehabilitation; pediatric rehabilitation; spinal cord injury rehabilitation; stroke rehabilitation; swallowing disorders; and traumatic brain injury rehabilitation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
