{"title":"Ischemic Proliferative Retinopathy in a Korean Patient with Cutis Marmorata Telangiectatica Congenita: A Case Report.","authors":"Min-Ji Kim, Sang Jin Kim","doi":"10.3341/kjo.2022.0107","DOIUrl":null,"url":null,"abstract":"Dear Editor, Cutis marmorata telangiectatica congenita (CMTC) is a rare congenital vascular anomaly, clinically diagnosed based on cutaneous features [1]. It is characterized by congenital persistent reticular erythema, that does not respond to local warming, and the absence of venectasisa within skin lesions. Histopathological examination revealed dilation of the veins and capillaries within the dermal layer of the skin [2]. Systemic manifestations related to CMTC include body asymmetry, syndactyly, neurological disorders, and ocular abnormalities [3]. Ocular abnormalities include glaucoma, retinal vascular abnormalities, retinal perfusion defects, and retinal detachments [4,5]. Herein, we report a case of ischemic proliferative retinopathy in a Korean patient with CMTC. The Institutional Review Board of Samsung Medical Center waived the need for informed consent (No. 2022-02-058). A 1-month-old Korean male patient, diagnosed with CMTC, was referred to the retina clinic for evaluation of accompanying ophthalmic abnormalities. The patient was born via Cesarean section due to oligohydramnios at 38 weeks of gestation and weighed 2.3 kg. After birth, tachypnea and cyanosis were observed, and the patient was admitted to the neonatal intensive care unit. Echocardiography revealed pulmonary hypertension. On physical examination performed at the time of admission, pinkish blue colored reticular erythema was observed on the face, upper extremities, and lower extremities, and CMTC was diagnosed based on characteristic clinical f indings (Fig. 1A, 1B). On anterior segment slit-lamp examination, no abnormalities were observed in the cornea, iris, or lens. Fundus examination showed abnormally dilated retinal vessels with peripheral avascular retinas in both eyes and vitreous hemorrhage in the right eye (Fig. 1C, 1D). An examination under general anesthesia was performed, and intravenous fluorescein angiography revealed an extensive nonperfusion area and retinal neovascularization in both eyes (Fig. 1E-1H). Laser ablation of the avascular retina with laser indirect ophthalmoscope was performed on the nonperfusion areas of both eyes. After 1.5 months of laser photocoagulation, retinal hemorrhage was absorbed, and retinal neovascularization regressed completely. The patient died of pulmonary hypertension 3 months after laser photocoagulation, and no further follow-up was possible. Dedania et al. [5] reported variable ocular involvement with frequent retinal vascular abnormalities in patients with CMTC. Avascular retina was detected in six of nine patients and two patients showed retinal detachment. As ischemic proliferative retinopathy accompanied by CMTC may progress rapidly and can cause retinal detachment and blindness, the authors recommended prompt comprehensive ophthalmic evaluation in infants with suspected CMTC. In summary, we report the case of a Korean patient with ischemic proliferative retinopathy accompanied by CMTC treated with laser photocoagulation. To the best of our knowledge, this is the first reported case of ischemic proliferative retinopathy in a patient with CMTC in the Korean population. Our case emphasizes that ophthalmic examination should be performed when CMTC is suspected, and prompt fluorescein angiography and laser photocoagulation is required if retinal nonperfusion or neovascularization is identified.","PeriodicalId":17883,"journal":{"name":"Korean Journal of Ophthalmology : KJO","volume":"36 6","pages":"570-571"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/84/c5/kjo-2022-0107.PMC9745346.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Ophthalmology : KJO","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3341/kjo.2022.0107","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
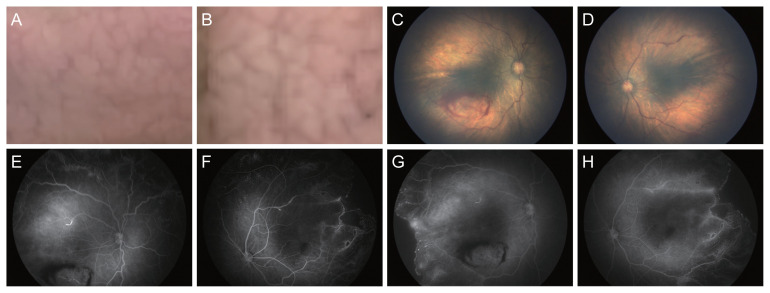
Dear Editor, Cutis marmorata telangiectatica congenita (CMTC) is a rare congenital vascular anomaly, clinically diagnosed based on cutaneous features [1]. It is characterized by congenital persistent reticular erythema, that does not respond to local warming, and the absence of venectasisa within skin lesions. Histopathological examination revealed dilation of the veins and capillaries within the dermal layer of the skin [2]. Systemic manifestations related to CMTC include body asymmetry, syndactyly, neurological disorders, and ocular abnormalities [3]. Ocular abnormalities include glaucoma, retinal vascular abnormalities, retinal perfusion defects, and retinal detachments [4,5]. Herein, we report a case of ischemic proliferative retinopathy in a Korean patient with CMTC. The Institutional Review Board of Samsung Medical Center waived the need for informed consent (No. 2022-02-058). A 1-month-old Korean male patient, diagnosed with CMTC, was referred to the retina clinic for evaluation of accompanying ophthalmic abnormalities. The patient was born via Cesarean section due to oligohydramnios at 38 weeks of gestation and weighed 2.3 kg. After birth, tachypnea and cyanosis were observed, and the patient was admitted to the neonatal intensive care unit. Echocardiography revealed pulmonary hypertension. On physical examination performed at the time of admission, pinkish blue colored reticular erythema was observed on the face, upper extremities, and lower extremities, and CMTC was diagnosed based on characteristic clinical f indings (Fig. 1A, 1B). On anterior segment slit-lamp examination, no abnormalities were observed in the cornea, iris, or lens. Fundus examination showed abnormally dilated retinal vessels with peripheral avascular retinas in both eyes and vitreous hemorrhage in the right eye (Fig. 1C, 1D). An examination under general anesthesia was performed, and intravenous fluorescein angiography revealed an extensive nonperfusion area and retinal neovascularization in both eyes (Fig. 1E-1H). Laser ablation of the avascular retina with laser indirect ophthalmoscope was performed on the nonperfusion areas of both eyes. After 1.5 months of laser photocoagulation, retinal hemorrhage was absorbed, and retinal neovascularization regressed completely. The patient died of pulmonary hypertension 3 months after laser photocoagulation, and no further follow-up was possible. Dedania et al. [5] reported variable ocular involvement with frequent retinal vascular abnormalities in patients with CMTC. Avascular retina was detected in six of nine patients and two patients showed retinal detachment. As ischemic proliferative retinopathy accompanied by CMTC may progress rapidly and can cause retinal detachment and blindness, the authors recommended prompt comprehensive ophthalmic evaluation in infants with suspected CMTC. In summary, we report the case of a Korean patient with ischemic proliferative retinopathy accompanied by CMTC treated with laser photocoagulation. To the best of our knowledge, this is the first reported case of ischemic proliferative retinopathy in a patient with CMTC in the Korean population. Our case emphasizes that ophthalmic examination should be performed when CMTC is suspected, and prompt fluorescein angiography and laser photocoagulation is required if retinal nonperfusion or neovascularization is identified.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
