Hristo Kirov, Tulio Caldonazo, Katia Audisio, Mohamed Rahouma, N Bryce Robinson, Gianmarco Cancelli, Giovanni J Soletti, Michelle Demetres, Mudathir Ibrahim, Gloria Faerber, Mario Gaudino, Torsten Doenst
{"title":"Association of liver dysfunction with outcomes after cardiac surgery-a meta-analysis.","authors":"Hristo Kirov, Tulio Caldonazo, Katia Audisio, Mohamed Rahouma, N Bryce Robinson, Gianmarco Cancelli, Giovanni J Soletti, Michelle Demetres, Mudathir Ibrahim, Gloria Faerber, Mario Gaudino, Torsten Doenst","doi":"10.1093/icvts/ivac280","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aim of this study was to perform a meta-analysis of studies reporting outcomes in patients with liver dysfunction addressed by the model of end-stage liver disease and Child-Turcotte-Pugh scores undergoing cardiac surgery.</p><p><strong>Methods: </strong>A systematic literature search was conducted to identify contemporary studies reporting short- and long-term outcomes in patients with liver dysfunction compared to patients with no or mild liver dysfunction undergoing cardiac surgery (stratified in high and low score group based on the study cut-offs). Primary outcome was perioperative mortality. Secondary outcomes were perioperative neurological events, prolonged ventilation, sepsis, bleeding and/or need for transfusion, acute kidney injury and long-term mortality.</p><p><strong>Results: </strong>A total of 33 studies with 48 891 patients were included. Compared with the low score group, being in the high score group was associated with significantly higher risk of perioperative mortality [odds ratio (OR) 3.72, 95% confidence interval (CI) 2.75-5.03, P < 0.001]. High score group was also associated with a significantly higher rate of perioperative neurological events (OR 1.49, 95% CI 1.30-1.71, P < 0.001), prolonged ventilation (OR 2.45, 95% CI 1.94-3.09, P < 0.001), sepsis (OR 3.88, 95% CI 2.07-7.26, P < 0.001), bleeding and/or need for transfusion (OR 1.95, 95% CI 1.43-2.64, P < 0.001), acute kidney injury (OR 3.84, 95% CI 2.12-6.98, P < 0.001) and long-term mortality (incidence risk ratio 1.29, 95% CI 1.14-1.46, P < 0.001).</p><p><strong>Conclusions: </strong>The analysis suggests that liver dysfunction in patients undergoing cardiac surgery is independently associated with higher risk of short and long-term mortality and also with an increased occurrence of various perioperative adverse events.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":"35 6","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9741516/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac280","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
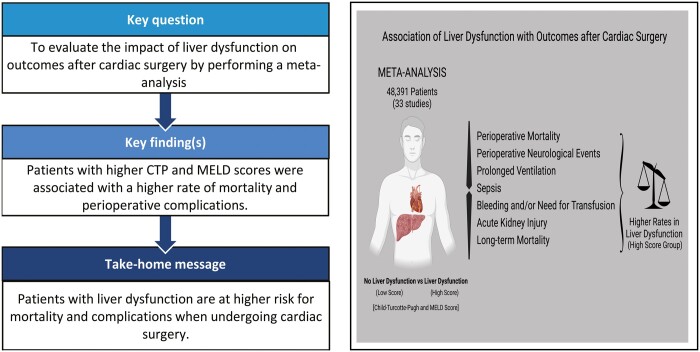
Objectives: The aim of this study was to perform a meta-analysis of studies reporting outcomes in patients with liver dysfunction addressed by the model of end-stage liver disease and Child-Turcotte-Pugh scores undergoing cardiac surgery.
Methods: A systematic literature search was conducted to identify contemporary studies reporting short- and long-term outcomes in patients with liver dysfunction compared to patients with no or mild liver dysfunction undergoing cardiac surgery (stratified in high and low score group based on the study cut-offs). Primary outcome was perioperative mortality. Secondary outcomes were perioperative neurological events, prolonged ventilation, sepsis, bleeding and/or need for transfusion, acute kidney injury and long-term mortality.
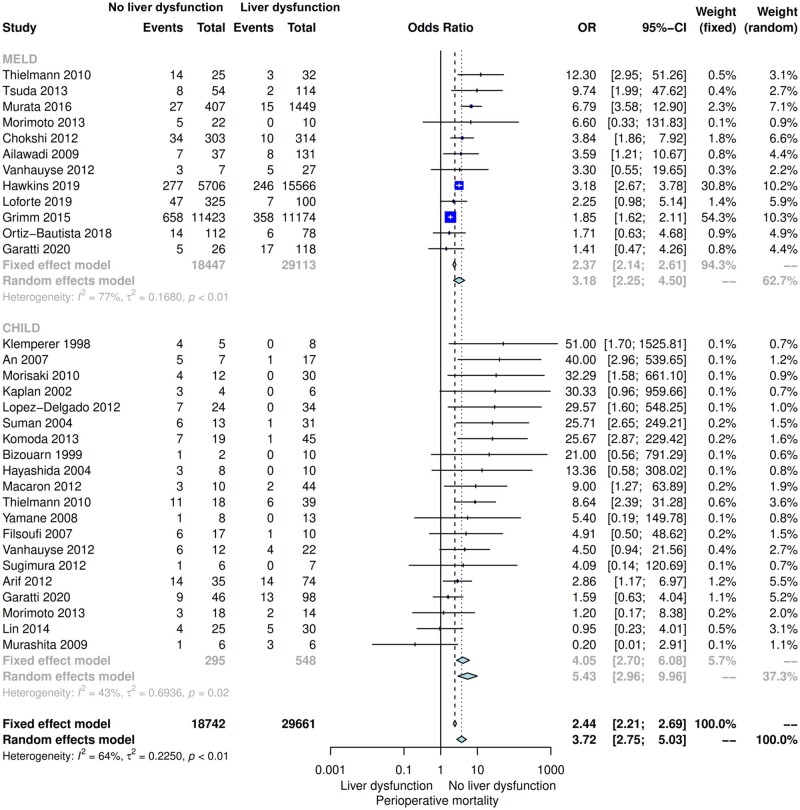
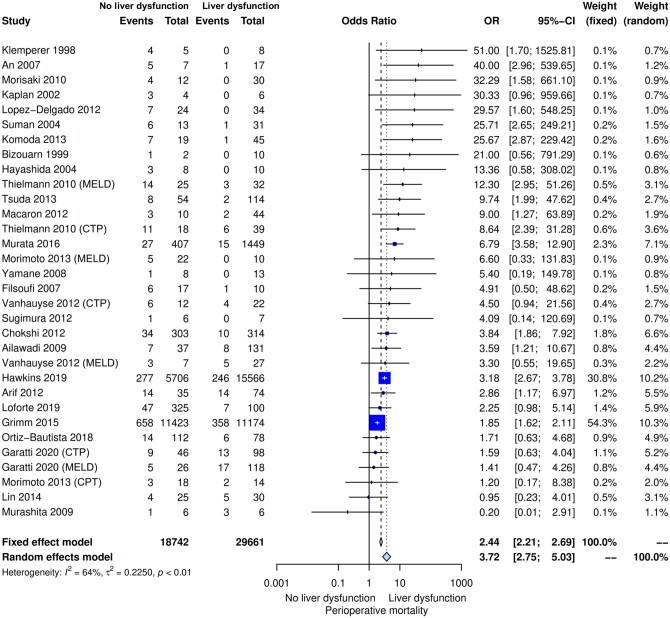
Results: A total of 33 studies with 48 891 patients were included. Compared with the low score group, being in the high score group was associated with significantly higher risk of perioperative mortality [odds ratio (OR) 3.72, 95% confidence interval (CI) 2.75-5.03, P < 0.001]. High score group was also associated with a significantly higher rate of perioperative neurological events (OR 1.49, 95% CI 1.30-1.71, P < 0.001), prolonged ventilation (OR 2.45, 95% CI 1.94-3.09, P < 0.001), sepsis (OR 3.88, 95% CI 2.07-7.26, P < 0.001), bleeding and/or need for transfusion (OR 1.95, 95% CI 1.43-2.64, P < 0.001), acute kidney injury (OR 3.84, 95% CI 2.12-6.98, P < 0.001) and long-term mortality (incidence risk ratio 1.29, 95% CI 1.14-1.46, P < 0.001).
Conclusions: The analysis suggests that liver dysfunction in patients undergoing cardiac surgery is independently associated with higher risk of short and long-term mortality and also with an increased occurrence of various perioperative adverse events.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
