Shane Shahrestani, Sammy Sayed, Tania Nasrollahi, Tasha Nasrollahi, Linda Huang, Erin McGillivray, William Chour, Andrew Foong, Shadi Dowlatshahi
{"title":"Association between frailty status and complications in patients undergoing surgical excision of malignant esophageal neoplasms.","authors":"Shane Shahrestani, Sammy Sayed, Tania Nasrollahi, Tasha Nasrollahi, Linda Huang, Erin McGillivray, William Chour, Andrew Foong, Shadi Dowlatshahi","doi":"10.20524/aog.2023.0825","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Research within the last decade highlights the patients' frailty status as an important predictor of esophageal cancer outcomes, but the literature evaluating frailty's role in these patients remains limited. We evaluated the role of frailty in patients undergoing resection of malignant esophageal neoplasms.</p><p><strong>Methods: </strong>We used the Nationwide Readmissions Database from 2016 and 2017 to identify patients who underwent excision of a malignant esophageal neoplasm. Patient frailty was queried using the Johns Hopkins Adjusted Clinical Groups frailty-defining diagnosis indicator. Propensity score matching identified 289 frail patients and 281 non-frail patients. Mann-Whitney U testing was performed and receiver operating characteristic (ROC) curves were created, following the creation of logistic regression models for predicting discharge disposition. The area under the curve (AUC) served as a proxy for model performance.</p><p><strong>Results: </strong>Frail patients had significantly more nonroutine discharges, longer inpatient lengths of stay, higher costs, more acute infections, posthemorrhagic anemia and deep vein thrombosis, and greater mortality (P<0.05). No significant differences were found between the 2 cohorts with respect to readmission rates, pulmonary embolism or dysphagia. Predictive models for patient discharge disposition demonstrated that frailty status in combination with age resulted in better ROC curves (AUC: 0.652) compared to models using age alone (AUC: 0.601).</p><p><strong>Conclusions: </strong>Frailty was found to be significantly correlated with higher rates of inpatient medical complications following esophagectomy. The inclusion of patient frailty status in predictive models for discharge disposition resulted in a better predictive capacity compared to those using age alone.</p>","PeriodicalId":7978,"journal":{"name":"Annals of Gastroenterology","volume":"36 5","pages":"517-523"},"PeriodicalIF":2.2000,"publicationDate":"2023-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a3/f7/AnnGastroenterol-36-517.PMC10433248.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20524/aog.2023.0825","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/7/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Research within the last decade highlights the patients' frailty status as an important predictor of esophageal cancer outcomes, but the literature evaluating frailty's role in these patients remains limited. We evaluated the role of frailty in patients undergoing resection of malignant esophageal neoplasms.
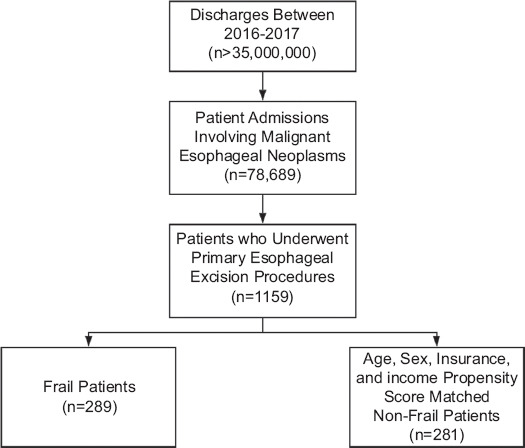
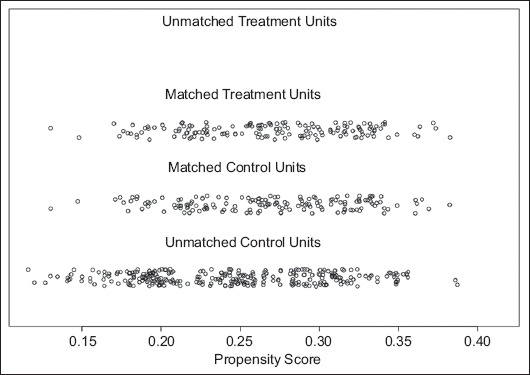
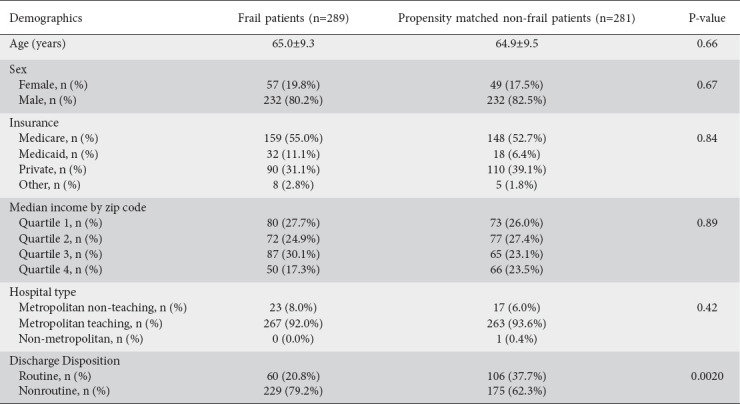
Methods: We used the Nationwide Readmissions Database from 2016 and 2017 to identify patients who underwent excision of a malignant esophageal neoplasm. Patient frailty was queried using the Johns Hopkins Adjusted Clinical Groups frailty-defining diagnosis indicator. Propensity score matching identified 289 frail patients and 281 non-frail patients. Mann-Whitney U testing was performed and receiver operating characteristic (ROC) curves were created, following the creation of logistic regression models for predicting discharge disposition. The area under the curve (AUC) served as a proxy for model performance.
Results: Frail patients had significantly more nonroutine discharges, longer inpatient lengths of stay, higher costs, more acute infections, posthemorrhagic anemia and deep vein thrombosis, and greater mortality (P<0.05). No significant differences were found between the 2 cohorts with respect to readmission rates, pulmonary embolism or dysphagia. Predictive models for patient discharge disposition demonstrated that frailty status in combination with age resulted in better ROC curves (AUC: 0.652) compared to models using age alone (AUC: 0.601).
Conclusions: Frailty was found to be significantly correlated with higher rates of inpatient medical complications following esophagectomy. The inclusion of patient frailty status in predictive models for discharge disposition resulted in a better predictive capacity compared to those using age alone.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
