Acquired HIV drug resistance among adults living with HIV receiving first-line antiretroviral therapy in Rwanda: A cross-sectional nationally representative survey.
Gentille Musengimana, Elysee Tuyishime, Athanase Kiromera, Samuel S Malamba, Augustin Mulindabigwi, Madjid R Habimana, Cyprien Baribwira, Muhayimpundu Ribakare, Savio D Habimana, Josh DeVos, Richard C N Mwesigwa, Eugenie Kayirangwa, Jules M Semuhore, Gallican N Rwibasira, Amitabh B Suthar, Eric Remera
{"title":"Acquired HIV drug resistance among adults living with HIV receiving first-line antiretroviral therapy in Rwanda: A cross-sectional nationally representative survey.","authors":"Gentille Musengimana, Elysee Tuyishime, Athanase Kiromera, Samuel S Malamba, Augustin Mulindabigwi, Madjid R Habimana, Cyprien Baribwira, Muhayimpundu Ribakare, Savio D Habimana, Josh DeVos, Richard C N Mwesigwa, Eugenie Kayirangwa, Jules M Semuhore, Gallican N Rwibasira, Amitabh B Suthar, Eric Remera","doi":"10.1177/13596535221102690","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>We assessed the prevalence of acquired HIV drug resistance (HIVDR) and associated factors among patients receiving first-line antiretroviral therapy (ART) in Rwanda.</p><p><strong>Methods: </strong>This cross-sectional study included 702 patients receiving first-line ART for at least 6 months with last viral load (VL) results ≥1000 copies/mL. Blood plasma samples were subjected to VL testing; specimens with unsuppressed VL were genotyped to identify HIVDR-associated mutations. Data were analysed using STATA/SE.</p><p><strong>Results: </strong>Median time on ART was 86.4 months (interquartile range [IQR], 44.8-130.2 months), and median CD4 count at ART initiation was 311 cells/mm<sup>3</sup> (IQR, 197-484 cells/mm<sup>3</sup>). Of 414 (68.2%) samples with unsuppressed VL, 378 (88.3%) were genotyped. HIVDR included 347 (90.4%) non-nucleoside reverse transcriptase inhibitor- (NNRTI), 291 (75.5%) nucleoside reverse transcriptase inhibitor- (NRTI) and 13 (3.5%) protease inhibitor (PI) resistance-associated mutations. The most common HIVDR mutations were K65R (22.7%), M184V (15.4%) and D67N (9.8%) for NRTIs and K103N (34.4%) and Y181C/I/V/YC (7%) for NNRTIs. Independent predictors of acquired HIVDR included current ART regimen of zidovudine + lamivudine + nevirapine (adjusted odds ratio [aOR], 3.333 [95% confidence interval (CI): 1.022-10.870]; p = 0.046) for NRTI resistance and current ART regimen of tenofovir + emtricitabine + nevirapine (aOR, 0.148 [95% CI: 0.028-0.779]; p = 0.025), zidovudine + lamivudine + efavirenz (aOR, 0.105 [95% CI: 0.016-0.693]; p = 0.020) and zidovudine + lamivudine + nevirapine (aOR, 0.259 [95% CI: 0.084-0.793]; p = 0.019) for NNRTI resistance. History of ever switching ART regimen was associated with NRTI resistance (aOR, 2.53 [95% CI: 1.198-5.356]; <i>p</i> = 0.016) and NNRTI resistance (aOR, 3.23 [95% CI: 1.435-7.278], p = 0.005).</p><p><strong>Conclusion: </strong>The prevalence of acquired HIV drug resistance (HIVDR) was high among patient failing to re-suppress VL and was associated with current ART regimen and ever switching ART regimen. The findings of this study support the current WHO guidelines recommending that patients on an NNRTI-based regimen should be switched based on a single viral load test and suggests that national HIV VL monitoring of patients receiving ART has prevented long-term treatment failure that would result in the accumulation of TAMs and potential loss of efficacy of all NRTI used in second-line ART as the backbone in combination with either dolutegravir or boosted PIs.</p>","PeriodicalId":8364,"journal":{"name":"Antiviral Therapy","volume":"27 3","pages":"13596535221102690"},"PeriodicalIF":2.3000,"publicationDate":"2022-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/80/71/nihms-1812025.PMC9263597.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antiviral Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/13596535221102690","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: We assessed the prevalence of acquired HIV drug resistance (HIVDR) and associated factors among patients receiving first-line antiretroviral therapy (ART) in Rwanda.
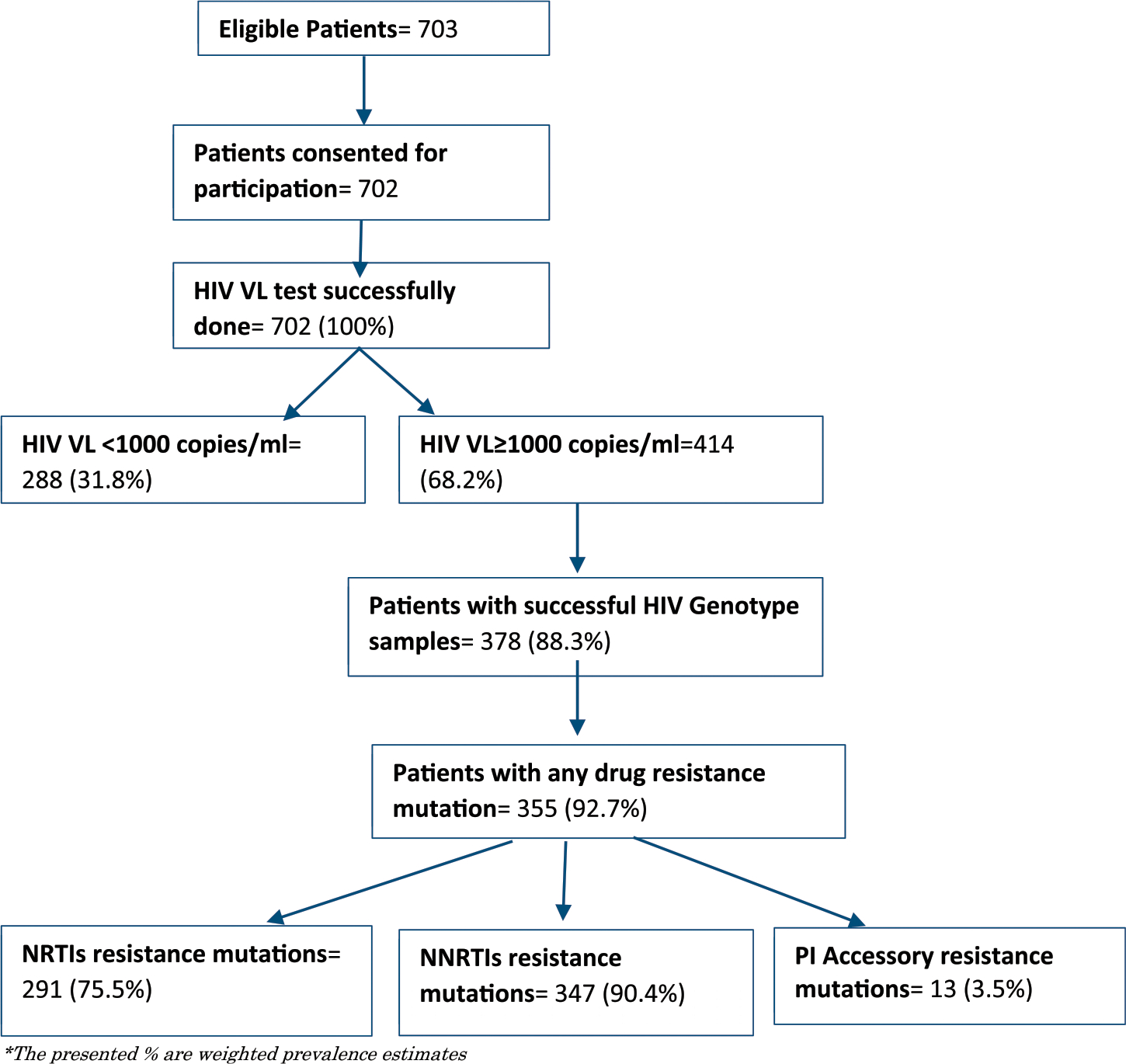
Methods: This cross-sectional study included 702 patients receiving first-line ART for at least 6 months with last viral load (VL) results ≥1000 copies/mL. Blood plasma samples were subjected to VL testing; specimens with unsuppressed VL were genotyped to identify HIVDR-associated mutations. Data were analysed using STATA/SE.
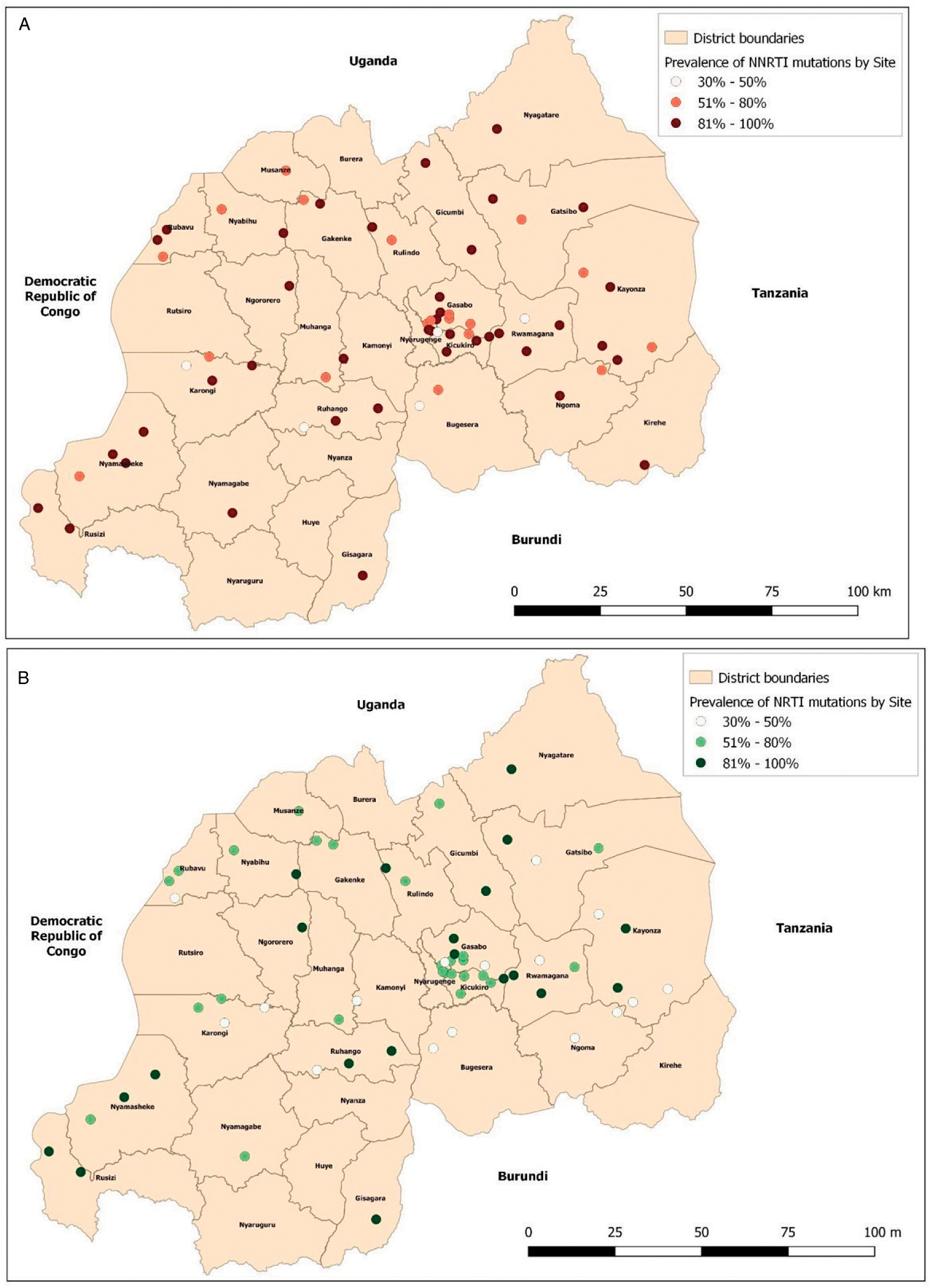
Results: Median time on ART was 86.4 months (interquartile range [IQR], 44.8-130.2 months), and median CD4 count at ART initiation was 311 cells/mm3 (IQR, 197-484 cells/mm3). Of 414 (68.2%) samples with unsuppressed VL, 378 (88.3%) were genotyped. HIVDR included 347 (90.4%) non-nucleoside reverse transcriptase inhibitor- (NNRTI), 291 (75.5%) nucleoside reverse transcriptase inhibitor- (NRTI) and 13 (3.5%) protease inhibitor (PI) resistance-associated mutations. The most common HIVDR mutations were K65R (22.7%), M184V (15.4%) and D67N (9.8%) for NRTIs and K103N (34.4%) and Y181C/I/V/YC (7%) for NNRTIs. Independent predictors of acquired HIVDR included current ART regimen of zidovudine + lamivudine + nevirapine (adjusted odds ratio [aOR], 3.333 [95% confidence interval (CI): 1.022-10.870]; p = 0.046) for NRTI resistance and current ART regimen of tenofovir + emtricitabine + nevirapine (aOR, 0.148 [95% CI: 0.028-0.779]; p = 0.025), zidovudine + lamivudine + efavirenz (aOR, 0.105 [95% CI: 0.016-0.693]; p = 0.020) and zidovudine + lamivudine + nevirapine (aOR, 0.259 [95% CI: 0.084-0.793]; p = 0.019) for NNRTI resistance. History of ever switching ART regimen was associated with NRTI resistance (aOR, 2.53 [95% CI: 1.198-5.356]; p = 0.016) and NNRTI resistance (aOR, 3.23 [95% CI: 1.435-7.278], p = 0.005).
Conclusion: The prevalence of acquired HIV drug resistance (HIVDR) was high among patient failing to re-suppress VL and was associated with current ART regimen and ever switching ART regimen. The findings of this study support the current WHO guidelines recommending that patients on an NNRTI-based regimen should be switched based on a single viral load test and suggests that national HIV VL monitoring of patients receiving ART has prevented long-term treatment failure that would result in the accumulation of TAMs and potential loss of efficacy of all NRTI used in second-line ART as the backbone in combination with either dolutegravir or boosted PIs.
期刊介绍:
Antiviral Therapy (an official publication of the International Society of Antiviral Research) is an international, peer-reviewed journal devoted to publishing articles on the clinical development and use of antiviral agents and vaccines, and the treatment of all viral diseases. Antiviral Therapy is one of the leading journals in virology and infectious diseases.
The journal is comprehensive, and publishes articles concerning all clinical aspects of antiviral therapy. It features editorials, original research papers, specially commissioned review articles, letters and book reviews. The journal is aimed at physicians and specialists interested in clinical and basic research.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
