{"title":"Feasibility and safety of neck level IB-sparing radiotherapy in nasopharyngeal cancer: a long-term single institution analysis.","authors":"Dowook Kim, Bhumsuk Keam, Soon-Hyun Ahn, Chang Heon Choi, Hong-Gyun Wu","doi":"10.3857/roj.2022.00346","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Nasopharyngeal cancer (NPC) has a higher prevalence of regional nodal metastasis than other head and neck cancers; however, level IB lymph node involvement is rare. We evaluated the safety and feasibility of level IB-sparing radiotherapy (RT) for NPC patients.</p><p><strong>Materials and methods: </strong>We retrospectively reviewed 236 patients with NPC who underwent definitive intensity-modulated RT with or without chemotherapy between 2004 and 2018. Of them, 212 received IB-sparing RT, and 24 received non-IB-sparing RT. We conducted a propensity score matching analysis to compare treatment outcomes according to IB-sparing status. In addition, dosimetric analysis of the salivary glands was performed to identify the relationship between xerostomia and the IB-sparing RT.</p><p><strong>Results: </strong>The median follow-up duration was 78 months (range, 7 to 194 months). Local, regional, and distant recurrences were observed in 11.9%, 6.8%, and 16.1% of patients, respectively. Of the 16 patients with regional recurrence, 14 underwent IB-sparing RT. The most common site categorization of regional recurrence was level II (75%), followed by retropharyngeal lymph nodes (43.8%); however, there was no recurrence at level IB. In the matched cohorts, IB-sparing RT was not significantly related to treatment outcomes. However, IB-sparing RT patients received a significantly lower mean ipsilateral and contralateral submandibular glands doses (all, p < 0.001) and had a lower incidence of chronic xerostomia compared with non-IB-sparing RT patients (p = 0.006).</p><p><strong>Conclusion: </strong>Our results demonstrated that IB-sparing RT is sufficiently safe and feasible for treating NPC. To reduce the occurrence of xerostomia, IB-sparing RT should be considered without compromising target coverage.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"40 4","pages":"260-269"},"PeriodicalIF":2.2000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2c/94/roj-2022-00346.PMC9830035.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2022.00346","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
Purpose: Nasopharyngeal cancer (NPC) has a higher prevalence of regional nodal metastasis than other head and neck cancers; however, level IB lymph node involvement is rare. We evaluated the safety and feasibility of level IB-sparing radiotherapy (RT) for NPC patients.
Materials and methods: We retrospectively reviewed 236 patients with NPC who underwent definitive intensity-modulated RT with or without chemotherapy between 2004 and 2018. Of them, 212 received IB-sparing RT, and 24 received non-IB-sparing RT. We conducted a propensity score matching analysis to compare treatment outcomes according to IB-sparing status. In addition, dosimetric analysis of the salivary glands was performed to identify the relationship between xerostomia and the IB-sparing RT.
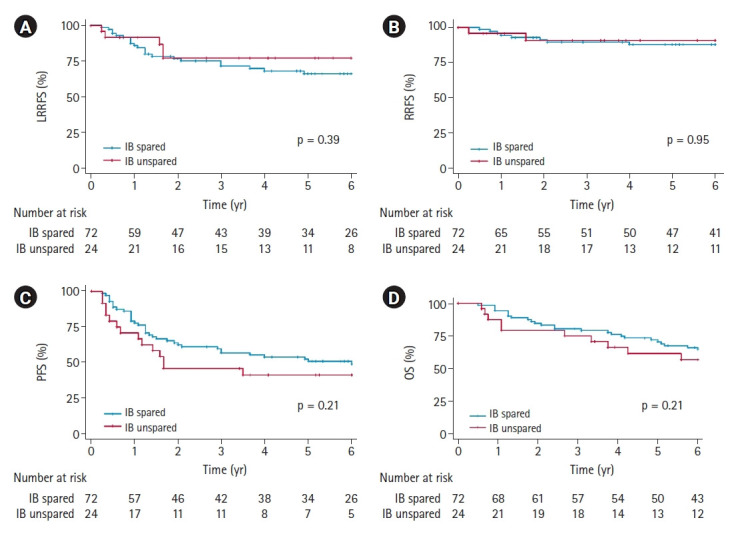
Results: The median follow-up duration was 78 months (range, 7 to 194 months). Local, regional, and distant recurrences were observed in 11.9%, 6.8%, and 16.1% of patients, respectively. Of the 16 patients with regional recurrence, 14 underwent IB-sparing RT. The most common site categorization of regional recurrence was level II (75%), followed by retropharyngeal lymph nodes (43.8%); however, there was no recurrence at level IB. In the matched cohorts, IB-sparing RT was not significantly related to treatment outcomes. However, IB-sparing RT patients received a significantly lower mean ipsilateral and contralateral submandibular glands doses (all, p < 0.001) and had a lower incidence of chronic xerostomia compared with non-IB-sparing RT patients (p = 0.006).
Conclusion: Our results demonstrated that IB-sparing RT is sufficiently safe and feasible for treating NPC. To reduce the occurrence of xerostomia, IB-sparing RT should be considered without compromising target coverage.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
