{"title":"Assessing the Incidence of New-onset Diabetes Mellitus with Statin Use: A Systematic Review of the Systematic Reviews and Meta-analyses.","authors":"Harmanjit Singh, Pallavi Sikarwar, Supreet Khurana, Jatin Sharma","doi":"10.17925/EE.2022.18.2.96","DOIUrl":null,"url":null,"abstract":"<p><p>Statin use has been linked with new-onset diabetes mellitus (NODM). In the present systematic review, we aimed to determine the incidence of NODM with statin use by assessing and summarizing the data generated by different systematic reviews and metaanalyses published on this topic. We conducted a systematic review of systematic reviews and meta-analyses using a pre-defined study protocol. Two authors independently performed a literature search using PubMed, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL) for studies reporting data on statin use and NODM incidence and screened and extracted data for the outcomes of interest. The Assessing the Methodological Auality of Systematic Reviews 2 (AMSTAR 2) checklist was used to evaluate the quality of the included systematic reviews and meta-analyses. The initial search yielded 621 potential records, and 16 relevant systematic reviews and meta-analyses were included in the present systematic review. The included studies showed an increase in the risk of NODM with statin use. In particular, rosuvastatin and atorvastatin were associated with NODM in many systematic reviews or meta-analyses; however, pravastatin and pitavastatin were found to be associated with lower or no risk. We observed a positive trend of development of NODM with statin use became more evident with advancing years as more number of studies were added. Intensive doses of statins and use in older subjects were found to be important risk factors for NODM. Finally, the quality assessment revealed that the included systematic reviews and metaanalyses were of critically low or low quality. We concluded that statin use carries a risk of causing NODM. Statins should not be discouraged in anticipation of NODM. However, glycaemic monitoring should be encouraged with the on-going statin therapy. Furthermore, clinical studies addressing the use of statins and the incidence of NODM as their primary objective should be planned.</p>","PeriodicalId":75231,"journal":{"name":"TouchREVIEWS in endocrinology","volume":"18 2","pages":"96-101"},"PeriodicalIF":0.0000,"publicationDate":"2022-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9835812/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"TouchREVIEWS in endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17925/EE.2022.18.2.96","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
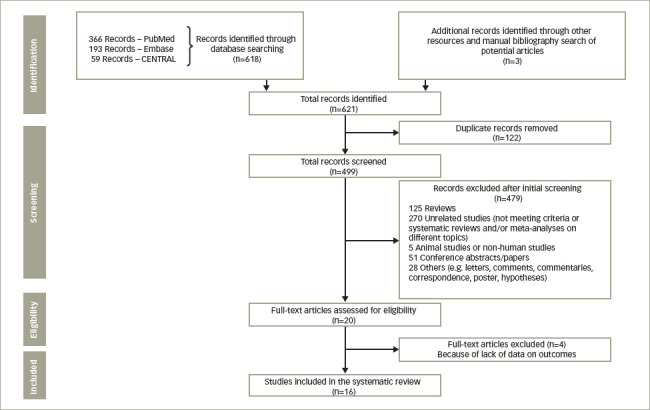
Statin use has been linked with new-onset diabetes mellitus (NODM). In the present systematic review, we aimed to determine the incidence of NODM with statin use by assessing and summarizing the data generated by different systematic reviews and metaanalyses published on this topic. We conducted a systematic review of systematic reviews and meta-analyses using a pre-defined study protocol. Two authors independently performed a literature search using PubMed, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL) for studies reporting data on statin use and NODM incidence and screened and extracted data for the outcomes of interest. The Assessing the Methodological Auality of Systematic Reviews 2 (AMSTAR 2) checklist was used to evaluate the quality of the included systematic reviews and meta-analyses. The initial search yielded 621 potential records, and 16 relevant systematic reviews and meta-analyses were included in the present systematic review. The included studies showed an increase in the risk of NODM with statin use. In particular, rosuvastatin and atorvastatin were associated with NODM in many systematic reviews or meta-analyses; however, pravastatin and pitavastatin were found to be associated with lower or no risk. We observed a positive trend of development of NODM with statin use became more evident with advancing years as more number of studies were added. Intensive doses of statins and use in older subjects were found to be important risk factors for NODM. Finally, the quality assessment revealed that the included systematic reviews and metaanalyses were of critically low or low quality. We concluded that statin use carries a risk of causing NODM. Statins should not be discouraged in anticipation of NODM. However, glycaemic monitoring should be encouraged with the on-going statin therapy. Furthermore, clinical studies addressing the use of statins and the incidence of NODM as their primary objective should be planned.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
