Lars K Markvardsen, Søren H Sindrup, Ingelise Christiansen, Aisha M Sheikh, Jakob V Holbech, Henning Andersen
{"title":"Standardized Tapering off Subcutaneous Immunoglobulin in Chronic Inflammatory Demyelinating Polyneuropathy.","authors":"Lars K Markvardsen, Søren H Sindrup, Ingelise Christiansen, Aisha M Sheikh, Jakob V Holbech, Henning Andersen","doi":"10.3233/JND-221615","DOIUrl":null,"url":null,"abstract":"Background: Attempting discontinuation of treatment in patients with chronic inflammatory demyelinating polyneuropathy (CIDP) is recommended. However, there is no evidence based regimen for tapering off subcutaneous immunoglobulin (SCIG). This trial investigated stepwise tapering off SCIG to detect remission and the lowest effective dosage. During tapering off, frequent vs less frequent clinical evaluation was compared. Methods: Patients with CIDP receiving a stable SCIG dosage followed a standardized tapering off regimen: 90%, 75%, 50%, 25% and 0% of the initial dose every 12th week, pending no deterioration occurred. In case of relapse during tapering off, the lowest effective dose was identified. Treatment with SCIG was registered for two years after participation. Disability score and grip strength were primary parameters. Participants were randomized to clinical evaluation every 6th week (frequent) or 12th week (less frequent). Results: Fifty-five patients were included of which thirty-five relapsed. Twenty patients (36%) were able to discontinue treatment without relapse. In relapsing patients, median dosage could be reduced by 10% (range, 0–75). After two years, 18 of 20 patients were still in remission without treatment. Frequent clinical evaluation did not detect deterioration more frequently than less frequent evaluation; RR 0.5 (95% CI, 0.2–1.2) (p = 0.17). Conclusion: In stable CIDP patients, SCIG could be completely tapered off in 36% of the patients and only in 10% of these patients relapse occurred during the following two years. More frequent evaluation was not superior to detect deterioration.","PeriodicalId":16536,"journal":{"name":"Journal of neuromuscular diseases","volume":"10 5","pages":"787-796"},"PeriodicalIF":3.4000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/36/5d/jnd-10-jnd221615.PMC10578281.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neuromuscular diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3233/JND-221615","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
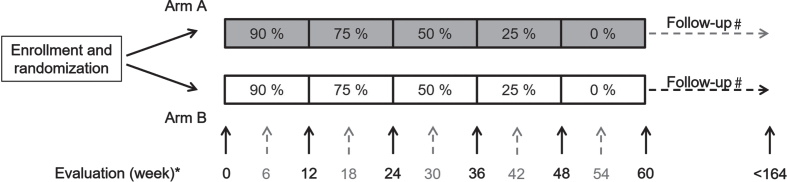
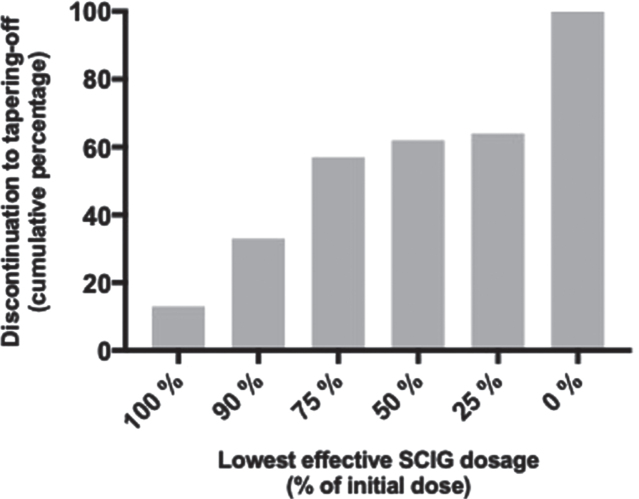
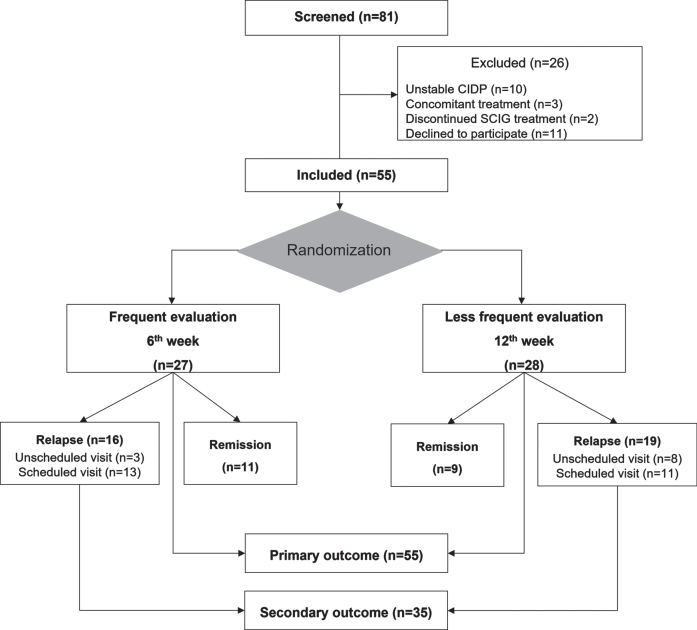
Background: Attempting discontinuation of treatment in patients with chronic inflammatory demyelinating polyneuropathy (CIDP) is recommended. However, there is no evidence based regimen for tapering off subcutaneous immunoglobulin (SCIG). This trial investigated stepwise tapering off SCIG to detect remission and the lowest effective dosage. During tapering off, frequent vs less frequent clinical evaluation was compared. Methods: Patients with CIDP receiving a stable SCIG dosage followed a standardized tapering off regimen: 90%, 75%, 50%, 25% and 0% of the initial dose every 12th week, pending no deterioration occurred. In case of relapse during tapering off, the lowest effective dose was identified. Treatment with SCIG was registered for two years after participation. Disability score and grip strength were primary parameters. Participants were randomized to clinical evaluation every 6th week (frequent) or 12th week (less frequent). Results: Fifty-five patients were included of which thirty-five relapsed. Twenty patients (36%) were able to discontinue treatment without relapse. In relapsing patients, median dosage could be reduced by 10% (range, 0–75). After two years, 18 of 20 patients were still in remission without treatment. Frequent clinical evaluation did not detect deterioration more frequently than less frequent evaluation; RR 0.5 (95% CI, 0.2–1.2) (p = 0.17). Conclusion: In stable CIDP patients, SCIG could be completely tapered off in 36% of the patients and only in 10% of these patients relapse occurred during the following two years. More frequent evaluation was not superior to detect deterioration.
期刊介绍:
The Journal of Neuromuscular Diseases aims to facilitate progress in understanding the molecular genetics/correlates, pathogenesis, pharmacology, diagnosis and treatment of acquired and genetic neuromuscular diseases (including muscular dystrophy, myasthenia gravis, spinal muscular atrophy, neuropathies, myopathies, myotonias and myositis). The journal publishes research reports, reviews, short communications, letters-to-the-editor, and will consider research that has negative findings. The journal is dedicated to providing an open forum for original research in basic science, translational and clinical research that will improve our fundamental understanding and lead to effective treatments of neuromuscular diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
