{"title":"Assessment of Carbon Monoxide in Exhaled Breath using the Smokerlyzer Handheld Machine: A Cross- Sectional Study.","authors":"Vinod K Ramani, Manohar Mhaske, Radheshyam Naik","doi":"10.1177/1179173X231184129","DOIUrl":null,"url":null,"abstract":"Introduction Nicotine dependence is known to be a chronic remitting and relapsing addictive disorder. Among cancer patients who smoke, nicotine addiction has been found to be more when compared with smoking healthy individuals. Smokerlyzer machine can be used to test smoking substance use and de-addiction services can be provided at Preventive Oncology units. The objectives of the study include: (i) To assess eCO using a Smokerlyzer hand-held machine and correlate it with the smoking status, (ii) To assess the cut-off value for smoking use, and discusses the benefits of this method. Methods In this cross-sectional study, healthy individuals at the workplace were tested for exhaled CO (eCO), which is used as a biological marker for monitoring the tobacco smoking. We discuss the feasibility of testing and its implications for cancer patients. The Bedfont EC50 Smokerlyzer machine was used to measure the concentration of CO in the end-tidal expired air. Results Among 643 study subjects, we found a statistically significant difference (P < .001) of median (IQR) eCO (measured in ppm) among smokers and non-smokers 2(1,5) vs 1(1,2). A significant and moderate positive correlation (Spearman rank correlation coefficient: .463) was observed between eCO and subjects who used cigarettes (measured in pack years). The ROC curve shows a cut off value for eCO as 2.5 with sensitivity 43.6% and 1 – specificity 2.76% (Specificity: 97.24%), which was rounded to 3. The area under the curve is 74.9%, which indicates a moderate discrimination performance of the test. The diagnostic accuracy of the test is 82.89%, which shows the proportion of correct test results. Conclusion Estimating eCO in health care settings will enable monitoring the smoking substance use which has important impact on clinical outcomes. In cancer hospitals, when the goal is complete abstinence a stringent CO cutoff in the range of 3-4 ppm should be used.","PeriodicalId":43361,"journal":{"name":"Tobacco Use Insights","volume":"16 ","pages":"1179173X231184129"},"PeriodicalIF":2.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1b/6b/10.1177_1179173X231184129.PMC10293515.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Tobacco Use Insights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179173X231184129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
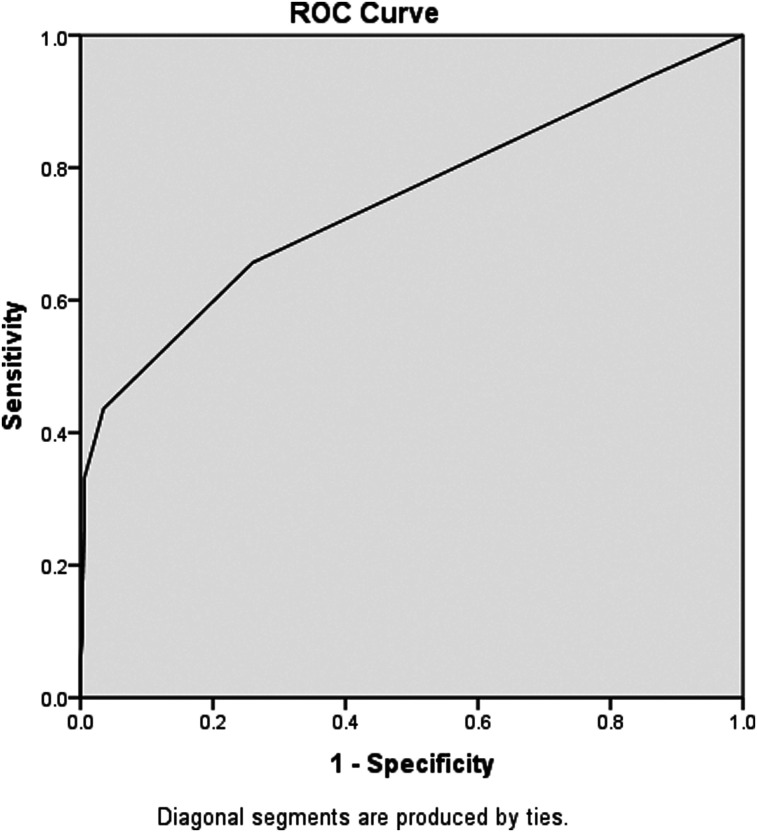
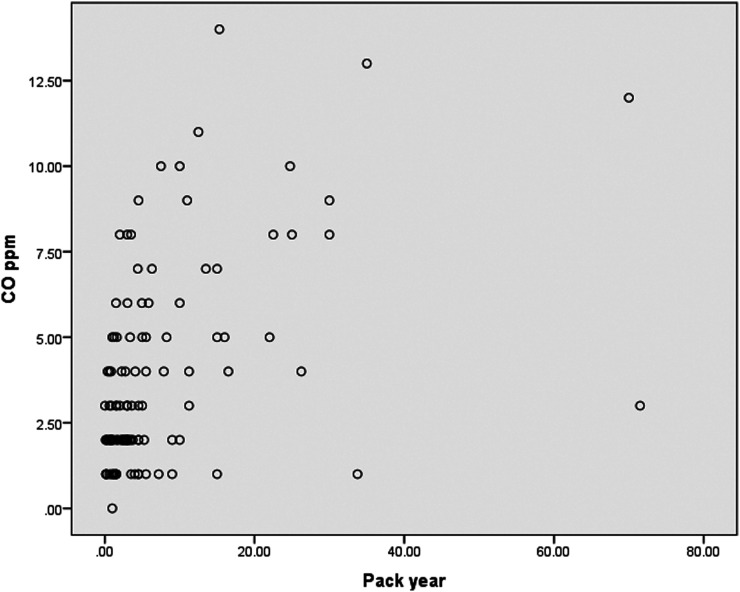
Introduction Nicotine dependence is known to be a chronic remitting and relapsing addictive disorder. Among cancer patients who smoke, nicotine addiction has been found to be more when compared with smoking healthy individuals. Smokerlyzer machine can be used to test smoking substance use and de-addiction services can be provided at Preventive Oncology units. The objectives of the study include: (i) To assess eCO using a Smokerlyzer hand-held machine and correlate it with the smoking status, (ii) To assess the cut-off value for smoking use, and discusses the benefits of this method. Methods In this cross-sectional study, healthy individuals at the workplace were tested for exhaled CO (eCO), which is used as a biological marker for monitoring the tobacco smoking. We discuss the feasibility of testing and its implications for cancer patients. The Bedfont EC50 Smokerlyzer machine was used to measure the concentration of CO in the end-tidal expired air. Results Among 643 study subjects, we found a statistically significant difference (P < .001) of median (IQR) eCO (measured in ppm) among smokers and non-smokers 2(1,5) vs 1(1,2). A significant and moderate positive correlation (Spearman rank correlation coefficient: .463) was observed between eCO and subjects who used cigarettes (measured in pack years). The ROC curve shows a cut off value for eCO as 2.5 with sensitivity 43.6% and 1 – specificity 2.76% (Specificity: 97.24%), which was rounded to 3. The area under the curve is 74.9%, which indicates a moderate discrimination performance of the test. The diagnostic accuracy of the test is 82.89%, which shows the proportion of correct test results. Conclusion Estimating eCO in health care settings will enable monitoring the smoking substance use which has important impact on clinical outcomes. In cancer hospitals, when the goal is complete abstinence a stringent CO cutoff in the range of 3-4 ppm should be used.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
