{"title":"A Patient with Transverse Colon Cancer Complicated by Cowden Syndrome Administered FOLFOXIRI + Bevacizumab Therapy.","authors":"Kazuhiro Takehara, Yoichi Ishizaki, Kunihiko Nagakari, Masakazu Ohuchi, Masaki Fukunaga, Kazuhiro Sakamoto","doi":"10.1159/000529001","DOIUrl":null,"url":null,"abstract":"<p><p>Cowden syndrome is characterized by several clinical features related to tumorous lesions primarily consisting of systemic hamartomas. The mutation of a tumor suppressor gene, the <i>PTEN</i> gene, is etiologically involved. As gastrointestinal lesions, polyps of all digestive tracts involving the esophagus to rectum develop. In patients with Cowden syndrome, the risk of colorectal cancer may increase. However, the characteristics of colorectal cancer in these patients remain to be clarified and sufficient findings regarding chemotherapy have not been obtained. A 39-year-old man was treated with a colonic stent for colitis obstructive due to circumferential transverse colon carcinoma. After decompression, elective extended laparoscopic right hemicolectomy was performed. Preoperative systemic detailed examination revealed characteristic dermal/mucosal findings, polyposis of the upper digestive tract, and a thyroid tumor. On <i>PTEN</i> gene sequencing, a mutation was detected at codon 130 of exon 5, leading to a diagnosis of Cowden syndrome. Postoperative adjuvant chemotherapy was performed for 6 months, but recurrent peritoneal dissemination was observed 1 month after its completion. FOLFOXIRI + bevacizumab therapy was started. Transiently, a partial response was achieved in peritoneally disseminated nodes according to the RECIST. There was no increase in the volume of cancerous ascites. However, an increase in the volume of ascites and local relapse were noted at the completion of the tenth course. The regimen was switched to FOLFIRI + panitumumab, but peritoneal dissemination exacerbated and the patient died 18 months after surgery.</p>","PeriodicalId":9614,"journal":{"name":"Case Reports in Gastroenterology","volume":"17 1","pages":"56-63"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/78/e6/crg-2022-0017-0001-529001.PMC9891847.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000529001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
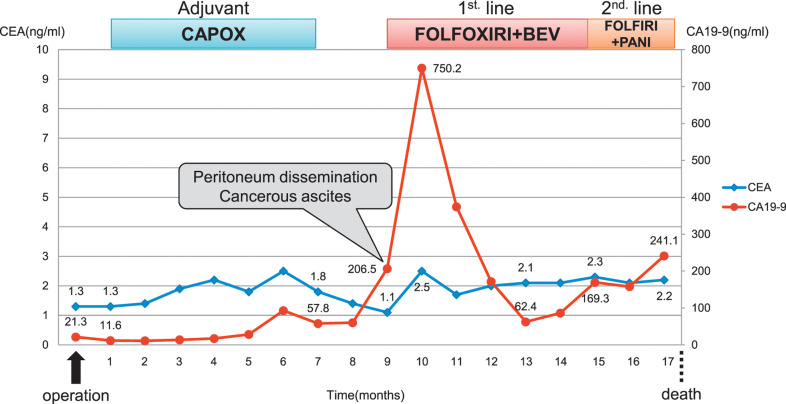
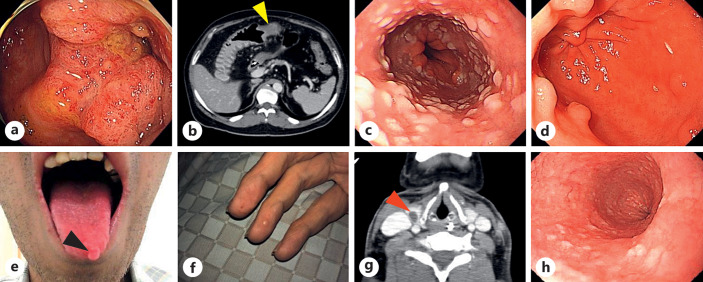
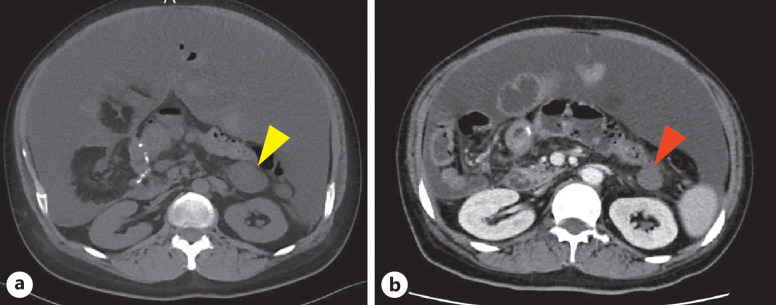
Cowden syndrome is characterized by several clinical features related to tumorous lesions primarily consisting of systemic hamartomas. The mutation of a tumor suppressor gene, the PTEN gene, is etiologically involved. As gastrointestinal lesions, polyps of all digestive tracts involving the esophagus to rectum develop. In patients with Cowden syndrome, the risk of colorectal cancer may increase. However, the characteristics of colorectal cancer in these patients remain to be clarified and sufficient findings regarding chemotherapy have not been obtained. A 39-year-old man was treated with a colonic stent for colitis obstructive due to circumferential transverse colon carcinoma. After decompression, elective extended laparoscopic right hemicolectomy was performed. Preoperative systemic detailed examination revealed characteristic dermal/mucosal findings, polyposis of the upper digestive tract, and a thyroid tumor. On PTEN gene sequencing, a mutation was detected at codon 130 of exon 5, leading to a diagnosis of Cowden syndrome. Postoperative adjuvant chemotherapy was performed for 6 months, but recurrent peritoneal dissemination was observed 1 month after its completion. FOLFOXIRI + bevacizumab therapy was started. Transiently, a partial response was achieved in peritoneally disseminated nodes according to the RECIST. There was no increase in the volume of cancerous ascites. However, an increase in the volume of ascites and local relapse were noted at the completion of the tenth course. The regimen was switched to FOLFIRI + panitumumab, but peritoneal dissemination exacerbated and the patient died 18 months after surgery.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
