Zylyftar Gorica, Kimberly McFarland, Conor N O'Neill, Jennifer Vanderbeck, Alexander R Vap
{"title":"Anatomic Shoulder Arthroplasty in the Setting of Concurrent or Prior Rotator Cuff Repair: A Systematic Review.","authors":"Zylyftar Gorica, Kimberly McFarland, Conor N O'Neill, Jennifer Vanderbeck, Alexander R Vap","doi":"10.1177/24715492231152733","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Reverse total shoulder arthroplasty (RSA) is the gold standard in management of osteoarthritis (OA) in the setting of rotator cuff pathology. However, there are significant complications associated with the procedure. An alternative option in the setting of a deficient rotator cuff may be to perform a repair prior to or concurrently with an anatomic total shoulder arthroplasty (aTSA).</p><p><strong>Methods: </strong>A systematic review was performed utilizing Preferred Reporting Items for Systematic Meta-Analyses (PRISMA) guidelines to evaluate outcomes in aTSA with concomitant or prior rotator cuff repair (RCR). Key outcomes were complication rate and subjective outcome scores.</p><p><strong>Results: </strong>Seven studies were included in the review. One study found a higher rate of total adverse events in the prior repair group (17% vs 7%, <i>P</i> = .01) while others found no significant difference. There was a nonstatistically significant increase in revision rates among patients with larger tears at time of repair. Prior repair groups were associated with a higher rate of re-tear in one study (13% vs 1%, <i>P</i> = .014). Concomitant repair was associated with a higher rate of loosening. In patients with prior repair, there was no statistical difference in strength, range of motion (ROM), simple shoulder test (SST), Single Assessment Numeric Evaluation (SANE), American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES), and visual analogue scale (VAS). In patients with concurrent repair, one study demonstrated a less drastic improvement in Hospital for Special Surgery (HSS) in \"moderate\" repairs as opposed to \"good\" repairs.</p><p><strong>Conclusions: </strong>Anatomic TSA is an appropriate treatment for glenohumeral OA in patients with a prior successful RCR and in younger patients with concurrent repair of small or medium tears.</p><p><strong>Level of evidence: </strong>Level III.</p>","PeriodicalId":73942,"journal":{"name":"Journal of shoulder and elbow arthroplasty","volume":"7 ","pages":"24715492231152733"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8a/21/10.1177_24715492231152733.PMC9896087.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of shoulder and elbow arthroplasty","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/24715492231152733","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Reverse total shoulder arthroplasty (RSA) is the gold standard in management of osteoarthritis (OA) in the setting of rotator cuff pathology. However, there are significant complications associated with the procedure. An alternative option in the setting of a deficient rotator cuff may be to perform a repair prior to or concurrently with an anatomic total shoulder arthroplasty (aTSA).
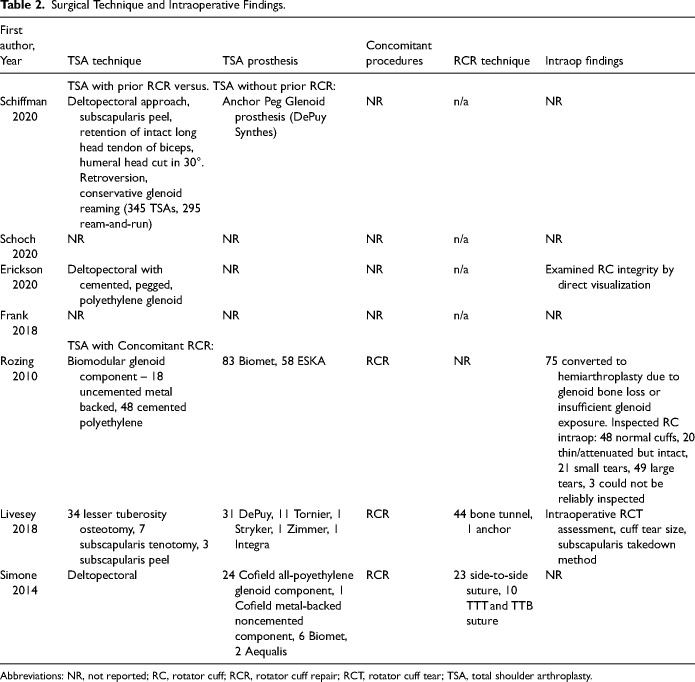
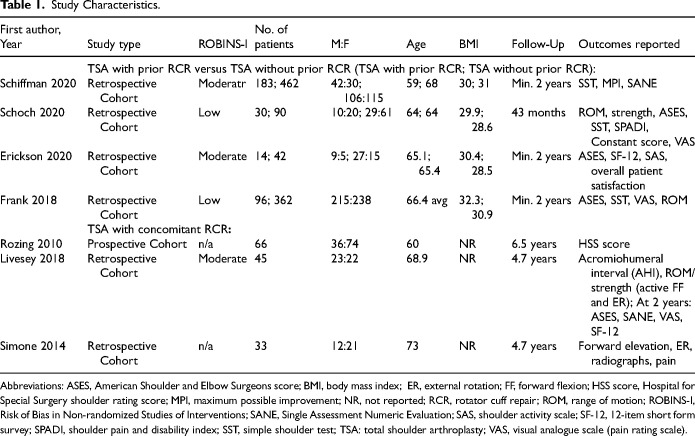
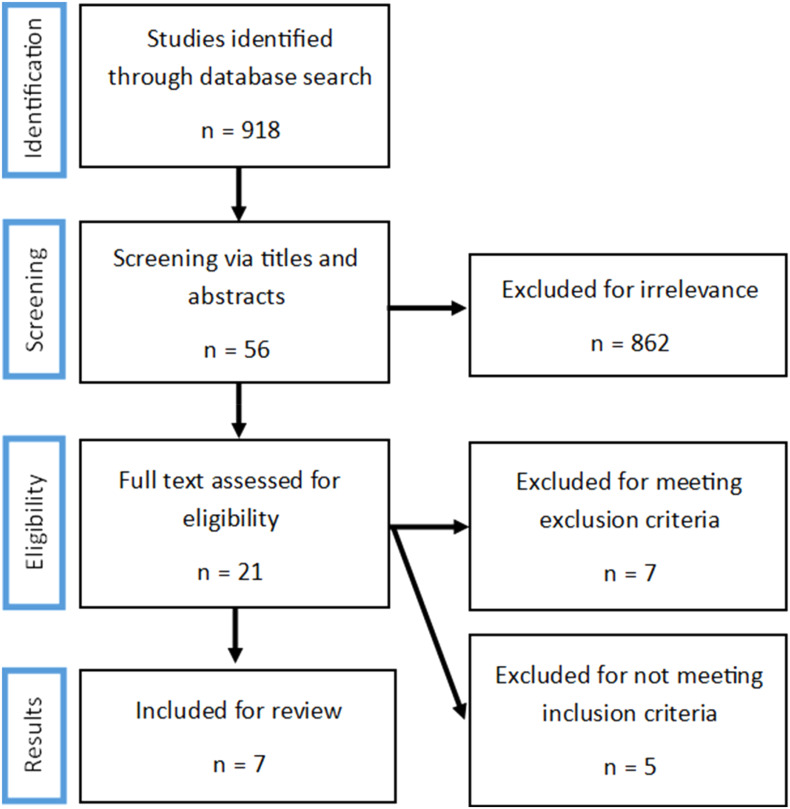
Methods: A systematic review was performed utilizing Preferred Reporting Items for Systematic Meta-Analyses (PRISMA) guidelines to evaluate outcomes in aTSA with concomitant or prior rotator cuff repair (RCR). Key outcomes were complication rate and subjective outcome scores.
Results: Seven studies were included in the review. One study found a higher rate of total adverse events in the prior repair group (17% vs 7%, P = .01) while others found no significant difference. There was a nonstatistically significant increase in revision rates among patients with larger tears at time of repair. Prior repair groups were associated with a higher rate of re-tear in one study (13% vs 1%, P = .014). Concomitant repair was associated with a higher rate of loosening. In patients with prior repair, there was no statistical difference in strength, range of motion (ROM), simple shoulder test (SST), Single Assessment Numeric Evaluation (SANE), American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form (ASES), and visual analogue scale (VAS). In patients with concurrent repair, one study demonstrated a less drastic improvement in Hospital for Special Surgery (HSS) in "moderate" repairs as opposed to "good" repairs.
Conclusions: Anatomic TSA is an appropriate treatment for glenohumeral OA in patients with a prior successful RCR and in younger patients with concurrent repair of small or medium tears.
背景:反向全肩关节置换术(RSA)是治疗骨关节炎(OA)在肩袖病理设置的金标准。然而,该手术有明显的并发症。另一种治疗肩袖缺陷的方法是在解剖性全肩关节置换术(aTSA)之前或同时进行修复。方法:利用系统荟萃分析(PRISMA)指南的首选报告项目进行系统评价,以评估aTSA合并或先前的肩袖修复(RCR)的结果。主要结局为并发症发生率和主观结局评分。结果:本综述纳入了7项研究。一项研究发现,先前修复组的总不良事件发生率更高(17% vs 7%, P = 0.01),而其他研究发现无显著差异。在修复时撕裂较大的患者中,翻修率增加无统计学意义。在一项研究中,先前的修复组与更高的再撕裂率相关(13% vs 1%, P = 0.014)。伴随修复与较高的松脱率相关。在先前进行修复的患者中,强度、活动范围(ROM)、简单肩关节测试(SST)、单一评估数值评估(SANE)、美国肩关节外科医生标准化肩关节评估表(ASES)和视觉模拟量表(VAS)无统计学差异。在同时进行修复的患者中,一项研究表明,在特殊外科医院(HSS),“中等”修复比“良好”修复的改善幅度较小。结论:解剖性TSA是一种合适的治疗方法,适用于先前RCR成功的患者和同时修复小或中等撕裂的年轻患者。证据等级:三级。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
