Cláudia Martins Marques Pinto, Marta Rodriguez, Madalena Souto Moura, Mariana Afonso, Pedro Bastos, Mário Dinis Ribeiro
{"title":"Gastric Metastatic Melanoma Mimicking a Hyperplastic Lesion.","authors":"Cláudia Martins Marques Pinto, Marta Rodriguez, Madalena Souto Moura, Mariana Afonso, Pedro Bastos, Mário Dinis Ribeiro","doi":"10.1159/000520211","DOIUrl":null,"url":null,"abstract":"A 56-year-old woman was submitted to an upper gastrointestinal endoscopy due to a recent history of epigastric pain. Endoscopic examination revealed a 20-mm 0-IIa type lesion in the great curvature of the proximal corpus with a hyperplastic appearance and a dark coloration area in one of the edges (Fig. 1, 2). Biopsy of the lesion was suggestive of mesenchymal proliferation and some cells with moderate cytologic atypia. The patient was then referred to our Endoscopy Department to undergo endoscopic resection. Due to the previous histological result, we decided to perform an endoscopic ultrasonography that showed thickening of the superficial layers of the mucosa. Endoscopic biopsies were repeated, and pathological evaluation revealed diffuse involvement of the lamina propria by a malignant neoplasm, composed of cells with nuclear pleomorphism and high mitotic rate, entrapping benign gastric glands. Immunohistochemistry showed diffuse positivity for melanocytic markers (PS100, SOX10 and MelanA) and negativity for cytokeratins, DOG-1 and CD45 (Fig. 3, 4). Given the clinical history of a malignant melanoma of the third left hand finger submitted to amputation 5 years before, a diagnosis of gastric metastasis of malignant melanoma was made. Thoraco-abdomino-pelvic computed tomography and PET scan showed no other metastasis. After multidisciplinary discussion, total gastrectomy was proposed to the patient given the location of the lesion (proximal corpus). During surgery, it was decided to perform an atypical gastrectomy following endoscopic tattoo. The histological specimen confirmed the diagnosis of malignant melanoma with free surgical margins. The patient is currently under clinical and imagiological (PET scan) surveillance. Malignant melanoma is a frequent source of metastases in the gastrointestinal tract [1]. The most frequent location is the small bowel followed by the colon and rectum; gastric metastases are rare [1, 2]. Metastatic disease is usually diagnosed within the first 3 years, but metasta-","PeriodicalId":51838,"journal":{"name":"GE Portuguese Journal of Gastroenterology","volume":"30 1","pages":"79-81"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1d/26/pjg-0030-0079.PMC9891148.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GE Portuguese Journal of Gastroenterology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000520211","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
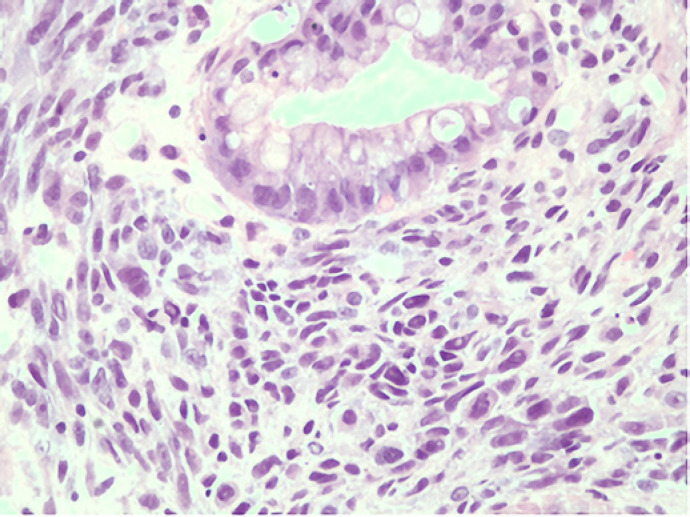
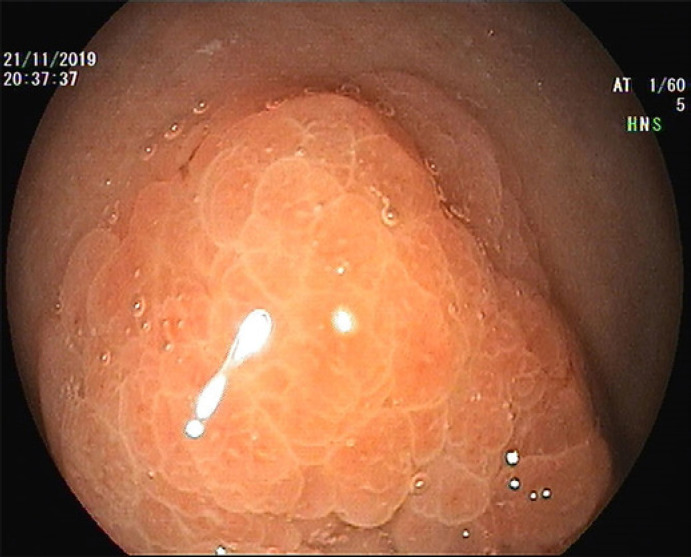
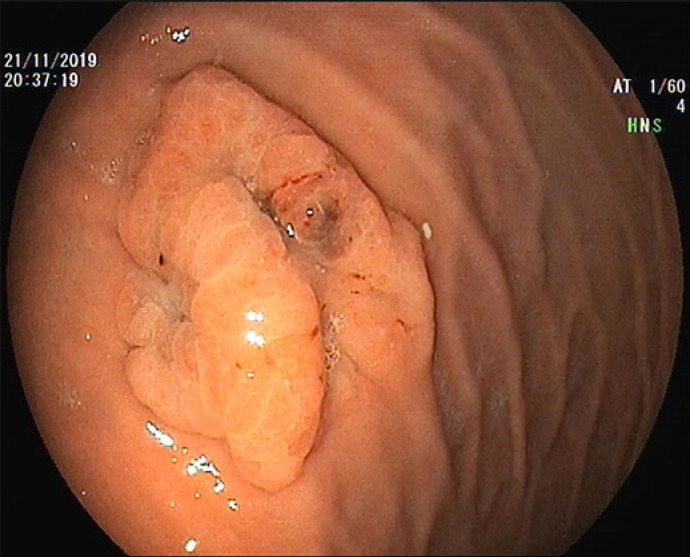
A 56-year-old woman was submitted to an upper gastrointestinal endoscopy due to a recent history of epigastric pain. Endoscopic examination revealed a 20-mm 0-IIa type lesion in the great curvature of the proximal corpus with a hyperplastic appearance and a dark coloration area in one of the edges (Fig. 1, 2). Biopsy of the lesion was suggestive of mesenchymal proliferation and some cells with moderate cytologic atypia. The patient was then referred to our Endoscopy Department to undergo endoscopic resection. Due to the previous histological result, we decided to perform an endoscopic ultrasonography that showed thickening of the superficial layers of the mucosa. Endoscopic biopsies were repeated, and pathological evaluation revealed diffuse involvement of the lamina propria by a malignant neoplasm, composed of cells with nuclear pleomorphism and high mitotic rate, entrapping benign gastric glands. Immunohistochemistry showed diffuse positivity for melanocytic markers (PS100, SOX10 and MelanA) and negativity for cytokeratins, DOG-1 and CD45 (Fig. 3, 4). Given the clinical history of a malignant melanoma of the third left hand finger submitted to amputation 5 years before, a diagnosis of gastric metastasis of malignant melanoma was made. Thoraco-abdomino-pelvic computed tomography and PET scan showed no other metastasis. After multidisciplinary discussion, total gastrectomy was proposed to the patient given the location of the lesion (proximal corpus). During surgery, it was decided to perform an atypical gastrectomy following endoscopic tattoo. The histological specimen confirmed the diagnosis of malignant melanoma with free surgical margins. The patient is currently under clinical and imagiological (PET scan) surveillance. Malignant melanoma is a frequent source of metastases in the gastrointestinal tract [1]. The most frequent location is the small bowel followed by the colon and rectum; gastric metastases are rare [1, 2]. Metastatic disease is usually diagnosed within the first 3 years, but metasta-
期刊介绍:
The ''GE Portuguese Journal of Gastroenterology'' (formerly Jornal Português de Gastrenterologia), founded in 1994, is the official publication of Sociedade Portuguesa de Gastrenterologia (Portuguese Society of Gastroenterology), Sociedade Portuguesa de Endoscopia Digestiva (Portuguese Society of Digestive Endoscopy) and Associação Portuguesa para o Estudo do Fígado (Portuguese Association for the Study of the Liver). The journal publishes clinical and basic research articles on Gastroenterology, Digestive Endoscopy, Hepatology and related topics. Review articles, clinical case studies, images, letters to the editor and other articles such as recommendations or papers on gastroenterology clinical practice are also considered. Only articles written in English are accepted.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
