Maria Moutafi, Dimitrios Afendoulis, Nikolaos Papagiannis, Athanasios Kartalis, Nikolaos Smyrnioudis
{"title":"Persistent Fever in a Patient With Mechanical Mitral Valve Replacement.","authors":"Maria Moutafi, Dimitrios Afendoulis, Nikolaos Papagiannis, Athanasios Kartalis, Nikolaos Smyrnioudis","doi":"10.4250/jcvi.2022.0026","DOIUrl":null,"url":null,"abstract":"https://e-jcvi.org A 77-year-old female patient with history of mechanical mitral valve replacement seven months before her presentation and paroxysmal atrial fibrillation was admitted to the emergency department with low-grade fever of three months duration, without taking any antibiotics during this period. She lived in a village of north Chios, but she denied any contact with contaminated dairy products or infected farm animals. Laboratory findings showed leukocytosis, thrombocytosis and increased C-reactive protein, erythrocyte sedimentation rate and ferritin and her electrocardiogram showed sinus rhythm. All blood cultures were negative. Neither transoesophageal echocardiogram (Movie 1) nor thoracic and abdominal computed tomography revealed abnormal findings. As neither cause of fever was recognized nor the diagnosis of infective endocarditis was confirmed based on 2 minor Duke’s criteria, a broad-spectrum antibiotic combination with ceftriaxone and vancomycin was administered initially. Serological tests for intracellular bacterial pathogens were performed and showed mildly increased immunoglobin (Ig) G and IgM antibodies for Coxiella burnetii (1:512 and 1:24, respectively). Based on it, the diagnosis of Q fever was considered quite possible and therapy with doxycycline and hydroxychloroquine was initiated. Despite the targeted therapy, she still suffered from fever 3 months later and a new serological test was collected, which revealed further increase of IgG and IgM antibodies (1:960 and 1:100, respectively). Moreover, a new computed tomography showed splenic septic emboli (Figure 1). A second transoesophageal echocardiogram revealed a 6x6 mm mitral vegetation, nonexistent at the previous one (Figures 2 and 3, Movies 2 and 3). Based on both the serological and echocardiographic findings, the diagnosis of Q fever endocarditis could be established as definite. The patient remains on doxycyxline-hydroxychloroquine combination therapy, while we highlighted the importance of adherence to therapy. She will be reevaluated in three months with new antibodies test according to the management strategy of Q fever.1)","PeriodicalId":15229,"journal":{"name":"Journal of Cardiovascular Imaging","volume":"31 1","pages":"68-70"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/54/36/jcvi-31-68.PMC9880343.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Imaging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4250/jcvi.2022.0026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
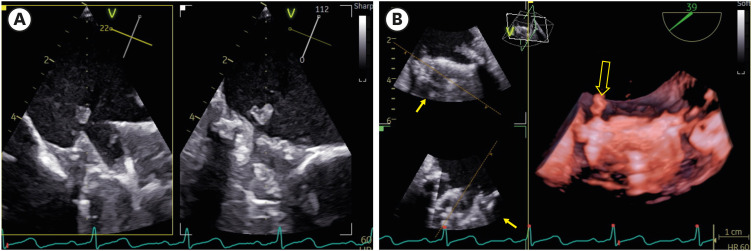
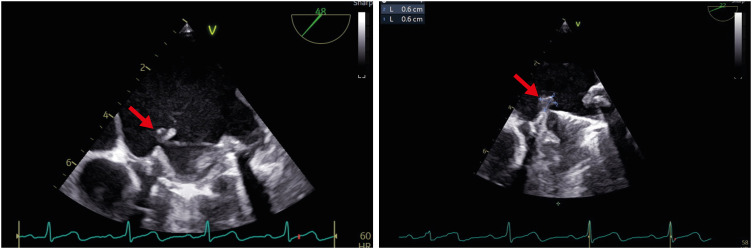
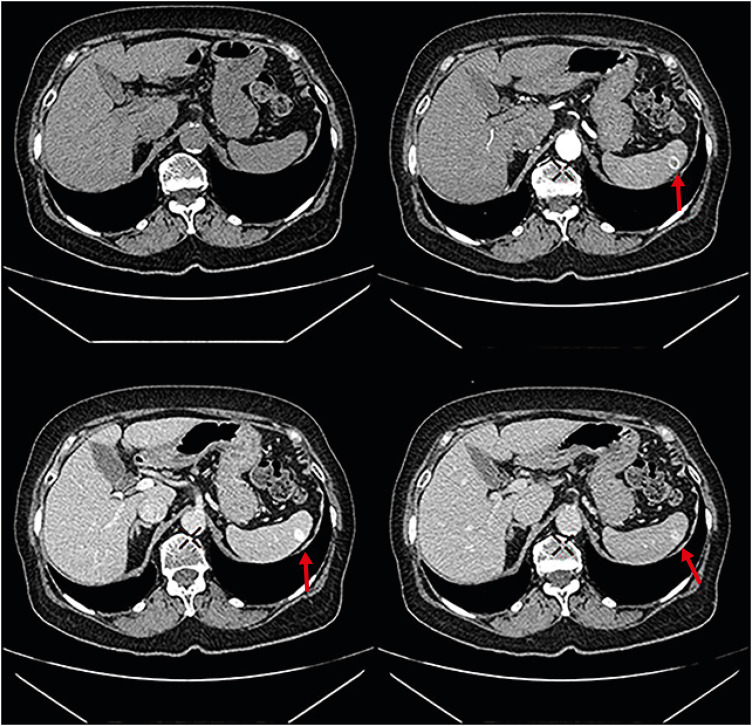
https://e-jcvi.org A 77-year-old female patient with history of mechanical mitral valve replacement seven months before her presentation and paroxysmal atrial fibrillation was admitted to the emergency department with low-grade fever of three months duration, without taking any antibiotics during this period. She lived in a village of north Chios, but she denied any contact with contaminated dairy products or infected farm animals. Laboratory findings showed leukocytosis, thrombocytosis and increased C-reactive protein, erythrocyte sedimentation rate and ferritin and her electrocardiogram showed sinus rhythm. All blood cultures were negative. Neither transoesophageal echocardiogram (Movie 1) nor thoracic and abdominal computed tomography revealed abnormal findings. As neither cause of fever was recognized nor the diagnosis of infective endocarditis was confirmed based on 2 minor Duke’s criteria, a broad-spectrum antibiotic combination with ceftriaxone and vancomycin was administered initially. Serological tests for intracellular bacterial pathogens were performed and showed mildly increased immunoglobin (Ig) G and IgM antibodies for Coxiella burnetii (1:512 and 1:24, respectively). Based on it, the diagnosis of Q fever was considered quite possible and therapy with doxycycline and hydroxychloroquine was initiated. Despite the targeted therapy, she still suffered from fever 3 months later and a new serological test was collected, which revealed further increase of IgG and IgM antibodies (1:960 and 1:100, respectively). Moreover, a new computed tomography showed splenic septic emboli (Figure 1). A second transoesophageal echocardiogram revealed a 6x6 mm mitral vegetation, nonexistent at the previous one (Figures 2 and 3, Movies 2 and 3). Based on both the serological and echocardiographic findings, the diagnosis of Q fever endocarditis could be established as definite. The patient remains on doxycyxline-hydroxychloroquine combination therapy, while we highlighted the importance of adherence to therapy. She will be reevaluated in three months with new antibodies test according to the management strategy of Q fever.1)



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
