Alexandros Rodolakis, Giovanni Scambia, François Planchamp, Maribel Acien, Attilio Di Spiezio Sardo, Martin Farrugia, Michael Grynberg, Maja Pakiz, Kitty Pavlakis, Nathalie Vermeulen, Gianfranco Zannoni, Ignacio Zapardiel, Kirsten Louise Tryde Macklon
{"title":"ESGO/ESHRE/ESGE Guidelines for the fertility-sparing treatment of patients with endometrial carcinoma<sup />.","authors":"Alexandros Rodolakis, Giovanni Scambia, François Planchamp, Maribel Acien, Attilio Di Spiezio Sardo, Martin Farrugia, Michael Grynberg, Maja Pakiz, Kitty Pavlakis, Nathalie Vermeulen, Gianfranco Zannoni, Ignacio Zapardiel, Kirsten Louise Tryde Macklon","doi":"10.1093/hropen/hoac057","DOIUrl":null,"url":null,"abstract":"<p><strong>Study question: </strong>How should fertility-sparing treatment of patients with endometrial carcinoma be performed?</p><p><strong>Summary answer: </strong>Forty-eight recommendations were formulated on fertility-sparing treatment of patients with endometrial carcinoma.</p><p><strong>What is known already: </strong>The standard surgical treatment of endometrial carcinoma consisting of total hysterectomy with bilateral salpingo-oophorectomy drastically affects the quality of life of patients and creates a challenge for clinicians. Recent evidence-based guidelines of the European Society of Gynaecological Oncology (ESGO), the European SocieTy for Radiotherapy & Oncology (ESTRO) and the European Society of Pathology (ESP) provide comprehensive guidelines on all relevant issues of diagnosis and treatment in endometrial carcinoma in a multidisciplinary setting. While addressing also work-up for fertility preservation treatments and the management and follow-up for fertility preservation, it was considered relevant to further extend the guidance on fertility-sparing treatment.</p><p><strong>Study design size duration: </strong>A collaboration was set up between the ESGO, the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), aiming to develop clinically relevant and evidence-based guidelines focusing on key aspects of fertility-sparing treatment in order to improve the quality of care for women with endometrial carcinoma across Europe and worldwide.</p><p><strong>Participants/materials setting methods: </strong>ESGO/ESHRE/ESGE nominated an international multidisciplinary development group consisting of practising clinicians and researchers who have demonstrated leadership and expertise in the care and research of endometrial carcinoma (11 experts across Europe). To ensure that the guidelines are evidence-based, the literature published since 2016, identified from a systematic search was reviewed and critically appraised. In the absence of any clear scientific evidence, judgement was based on the professional experience and consensus of the development group. The guidelines are thus based on the best available evidence and expert agreement. Prior to publication, the guidelines were reviewed by 95 independent international practitioners in cancer care delivery and patient representatives.</p><p><strong>Main results and the role of chance: </strong>The multidisciplinary development group formulated 48 recommendations in four sections; patient selection, tumour clinicopathological characteristics, treatment and special issues.</p><p><strong>Limitations reasons for caution: </strong>Of the 48 recommendations, none could be based on level I evidence and only 16 could be based on level II evidence, implicating that 66% of the recommendations are supported only by observational data, professional experience and consensus of the development group.</p><p><strong>Wider implications of the findings: </strong>These recommendations provide guidance to professionals caring for women with endometrial carcinoma, including but not limited to professionals in the field of gynaecological oncology, onco-fertility, reproductive surgery, endoscopy, conservative surgery and histopathology, and will help towards a holistic and multidisciplinary approach for this challenging clinical scenario.</p><p><strong>Study funding/competing interests: </strong>All costs relating to the development process were covered from ESGO, ESHRE and ESGE funds. There was no external funding of the development process or manuscript production. G.S. has reported grants from MSD Italia S.r.l., advisory boards for Storz, Bayer, Astrazeneca, Metronic, TESARO Bio Italy S.r.l and Johnson & Johnson, and honoraria for lectures from Clovis Oncology Italy S.r.l. M.G. has reported advisory boards for Gedeon Richter and Merck. The other authors have reported no conflicts of interest.</p><p><strong>Disclaimer: </strong><i>This document represents the views of ESHRE, ESGO and ESGE which are the result of consensus between the relevant stakeholders and where relevant based on the scientific evidence available at the time of preparation</i>. <i>The recommendations should be used for informational and educational purposes. They should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care nor exclusive of other methods of care reasonably directed to obtaining the same results. They do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type</i>.</p>","PeriodicalId":73264,"journal":{"name":"Human reproduction open","volume":"2023 1","pages":"hoac057"},"PeriodicalIF":11.1000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9900425/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Human reproduction open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/hropen/hoac057","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
Study question: How should fertility-sparing treatment of patients with endometrial carcinoma be performed?
Summary answer: Forty-eight recommendations were formulated on fertility-sparing treatment of patients with endometrial carcinoma.
What is known already: The standard surgical treatment of endometrial carcinoma consisting of total hysterectomy with bilateral salpingo-oophorectomy drastically affects the quality of life of patients and creates a challenge for clinicians. Recent evidence-based guidelines of the European Society of Gynaecological Oncology (ESGO), the European SocieTy for Radiotherapy & Oncology (ESTRO) and the European Society of Pathology (ESP) provide comprehensive guidelines on all relevant issues of diagnosis and treatment in endometrial carcinoma in a multidisciplinary setting. While addressing also work-up for fertility preservation treatments and the management and follow-up for fertility preservation, it was considered relevant to further extend the guidance on fertility-sparing treatment.
Study design size duration: A collaboration was set up between the ESGO, the European Society of Human Reproduction and Embryology (ESHRE) and the European Society for Gynaecological Endoscopy (ESGE), aiming to develop clinically relevant and evidence-based guidelines focusing on key aspects of fertility-sparing treatment in order to improve the quality of care for women with endometrial carcinoma across Europe and worldwide.
Participants/materials setting methods: ESGO/ESHRE/ESGE nominated an international multidisciplinary development group consisting of practising clinicians and researchers who have demonstrated leadership and expertise in the care and research of endometrial carcinoma (11 experts across Europe). To ensure that the guidelines are evidence-based, the literature published since 2016, identified from a systematic search was reviewed and critically appraised. In the absence of any clear scientific evidence, judgement was based on the professional experience and consensus of the development group. The guidelines are thus based on the best available evidence and expert agreement. Prior to publication, the guidelines were reviewed by 95 independent international practitioners in cancer care delivery and patient representatives.
Main results and the role of chance: The multidisciplinary development group formulated 48 recommendations in four sections; patient selection, tumour clinicopathological characteristics, treatment and special issues.
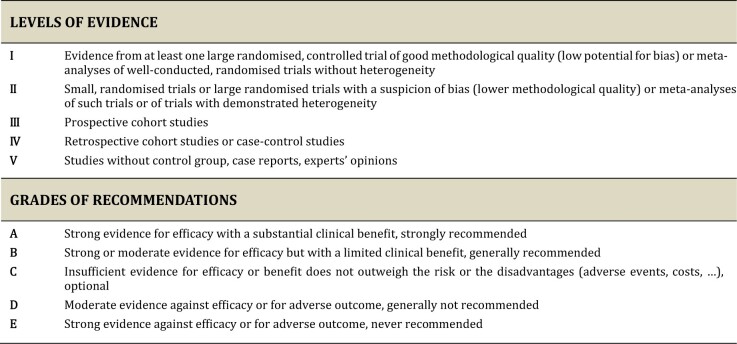
Limitations reasons for caution: Of the 48 recommendations, none could be based on level I evidence and only 16 could be based on level II evidence, implicating that 66% of the recommendations are supported only by observational data, professional experience and consensus of the development group.
Wider implications of the findings: These recommendations provide guidance to professionals caring for women with endometrial carcinoma, including but not limited to professionals in the field of gynaecological oncology, onco-fertility, reproductive surgery, endoscopy, conservative surgery and histopathology, and will help towards a holistic and multidisciplinary approach for this challenging clinical scenario.
Study funding/competing interests: All costs relating to the development process were covered from ESGO, ESHRE and ESGE funds. There was no external funding of the development process or manuscript production. G.S. has reported grants from MSD Italia S.r.l., advisory boards for Storz, Bayer, Astrazeneca, Metronic, TESARO Bio Italy S.r.l and Johnson & Johnson, and honoraria for lectures from Clovis Oncology Italy S.r.l. M.G. has reported advisory boards for Gedeon Richter and Merck. The other authors have reported no conflicts of interest.
Disclaimer: This document represents the views of ESHRE, ESGO and ESGE which are the result of consensus between the relevant stakeholders and where relevant based on the scientific evidence available at the time of preparation. The recommendations should be used for informational and educational purposes. They should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care nor exclusive of other methods of care reasonably directed to obtaining the same results. They do not replace the need for application of clinical judgement to each individual presentation, nor variations based on locality and facility type.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
