{"title":"COVID-19 Associated Fulminant Myocarditis in a Fully-Vaccinated Female: A Case Report with Clinical Follow-up.","authors":"Parham Samimisedeh, Fatemeh Sehati, Elmira Jafari Afshar","doi":"10.1177/11795476221147238","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Myocarditis is considered a serious adverse event after COVID-19 infection. The risk and severity of myocarditis after COVID-19 disease decreased significantly in the vaccinated population. We present a case of cardiac magnetic resonance proven fulminant myocarditis following COVID-19 disease in a young female who was previously vaccinated with 2 doses of the BIBP (Sinopharm) vaccine.</p><p><strong>Case summary: </strong>A 29-year-old female was referred to the hospital with acute chest pain, dyspnea, and nausea. Her electrocardiogram revealed ST-segment elevation in anterolateral leads with reciprocal changes in inferior leads. She was primarily diagnosed with ST-elevation myocardial infarction following spontaneous coronary artery dissection (SCAD) according to her age and gender. Her coronary angiography was normal. RT-PCR nasopharyngeal swab was positive for SARS-COV-2 infection. According to her history and excluding coronary artery diseases, she was clinically diagnosed with myocarditis and received corticosteroids, IVIG, and colchicine. She was discharged in a favorable condition after 11 days of hospitalization. Cardiac magnetic resonance imaging confirmed the diagnosis of myocarditis according to the updated lake Louise criteria. On her 4-month follow-up, she was asymptomatic, and her echocardiography showed improvement in biventricular function.</p><p><strong>Discussion: </strong>The diagnosis of myocarditis caused by COVID-19 infection may be challenging as the symptoms of myocarditis, and COVID-19 disease may overlap. It should be considered when patients have acute chest pain, palpitation, elevated cardiac biomarkers, and new abnormalities in ECG or echocardiography. Cardiac MRI is a non-invasive gold standard modality for diagnosing and follow-up of myocarditis and should be used in clinically suspected myocarditis. The long-term course of myocarditis following COVID-19 disease is still unclear, but some evidence suggests it may have a favorable mid-term outcome.</p>","PeriodicalId":10357,"journal":{"name":"Clinical Medicine Insights. Case Reports","volume":"16 ","pages":"11795476221147238"},"PeriodicalIF":0.6000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/51/58/10.1177_11795476221147238.PMC9912035.pdf","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights. Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11795476221147238","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Myocarditis is considered a serious adverse event after COVID-19 infection. The risk and severity of myocarditis after COVID-19 disease decreased significantly in the vaccinated population. We present a case of cardiac magnetic resonance proven fulminant myocarditis following COVID-19 disease in a young female who was previously vaccinated with 2 doses of the BIBP (Sinopharm) vaccine.
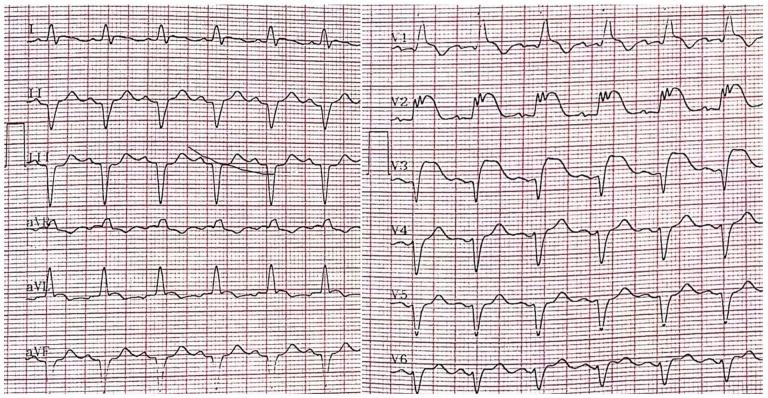
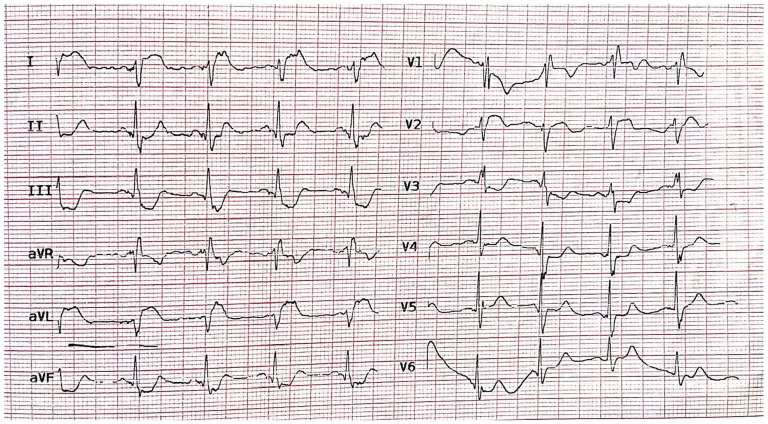
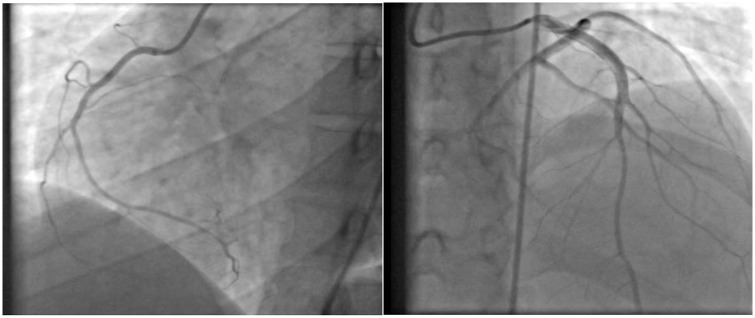
Case summary: A 29-year-old female was referred to the hospital with acute chest pain, dyspnea, and nausea. Her electrocardiogram revealed ST-segment elevation in anterolateral leads with reciprocal changes in inferior leads. She was primarily diagnosed with ST-elevation myocardial infarction following spontaneous coronary artery dissection (SCAD) according to her age and gender. Her coronary angiography was normal. RT-PCR nasopharyngeal swab was positive for SARS-COV-2 infection. According to her history and excluding coronary artery diseases, she was clinically diagnosed with myocarditis and received corticosteroids, IVIG, and colchicine. She was discharged in a favorable condition after 11 days of hospitalization. Cardiac magnetic resonance imaging confirmed the diagnosis of myocarditis according to the updated lake Louise criteria. On her 4-month follow-up, she was asymptomatic, and her echocardiography showed improvement in biventricular function.
Discussion: The diagnosis of myocarditis caused by COVID-19 infection may be challenging as the symptoms of myocarditis, and COVID-19 disease may overlap. It should be considered when patients have acute chest pain, palpitation, elevated cardiac biomarkers, and new abnormalities in ECG or echocardiography. Cardiac MRI is a non-invasive gold standard modality for diagnosing and follow-up of myocarditis and should be used in clinically suspected myocarditis. The long-term course of myocarditis following COVID-19 disease is still unclear, but some evidence suggests it may have a favorable mid-term outcome.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
