{"title":"Oncologic outcomes of segmentectomy for stage IA radiological solid-predominant lung cancer >2 cm in maximum tumour size.","authors":"Aritoshi Hattori, Takeshi Matsunaga, Mariko Fukui, Kazuya Takamochi, Shiaki Oh, Kenji Suzuki","doi":"10.1093/icvts/ivac246","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>We aimed to compare the outcomes of segmentectomy with those of lobectomy in clinical-stage IA radiological solid-predominant non-small-cell lung cancer (NSCLC) >2 cm in maximum tumour size.</p><p><strong>Methods: </strong>A retrospective review was performed for radiological solid-predominant NSCLC >2-3 cm in maximum tumour size with a ground-glass opacity component on thin-section computed tomography. Multivariable or propensity score-matched analyses were performed to control for confounders for survival. Overall survival (OS) was analysed using a Kaplan-Meier estimation.</p><p><strong>Results: </strong>Of the 215 eligible cases, segmentectomy and lobectomy were performed in 46 and 169 patients. Multivariable analysis revealed that standardized uptake value (hazard ratio: 1.148, 95% confidence interval: 1.032-1.276, P = 0.011) was an independently significant prognosticators of OS, while the operative mode was not associated (hazard ratio: 0.635, 95% confidence interval: 0.132-3.049, P = 0.570). The 5 y-OS was excellent and did not differ significantly between segmentectomy and lobectomy (95.5% vs 90.2%; P = 0.697), which was also shown in the propensity score analysis (96.8% vs 94.0%; P = 0.406), with a median follow-up time of 5.2 years. Locoregional recurrence was found in 2 (4.3%) segmentectomy and 13 (7.7%) lobectomy (P = 0.443). In the subgroup analysis stratified by solid component size, the 5 y-OS was similar between segmentectomy and lobectomy in the c-T1b and c-T1c groups, respectively [c-T1b (n = 163): 94.1% vs 91.8%; P = 0.887 and c-T1c (n = 52): 100% vs 84.9%; P = 0.197].</p><p><strong>Conclusions: </strong>Segmentectomy showed similar oncological results compared to lobectomy in solid-predominant NSCLC with a ground-glass opacity component >2-3 cm in maximum tumour size. More prospective randomized trials are needed to adequately expand the indication of anatomic segmentectomy for early-stage NSCLC.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":"35 6","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9725180/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac246","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 3
Abstract
Objectives: We aimed to compare the outcomes of segmentectomy with those of lobectomy in clinical-stage IA radiological solid-predominant non-small-cell lung cancer (NSCLC) >2 cm in maximum tumour size.
Methods: A retrospective review was performed for radiological solid-predominant NSCLC >2-3 cm in maximum tumour size with a ground-glass opacity component on thin-section computed tomography. Multivariable or propensity score-matched analyses were performed to control for confounders for survival. Overall survival (OS) was analysed using a Kaplan-Meier estimation.
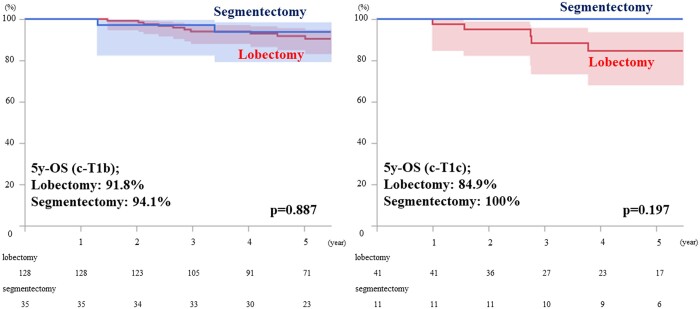
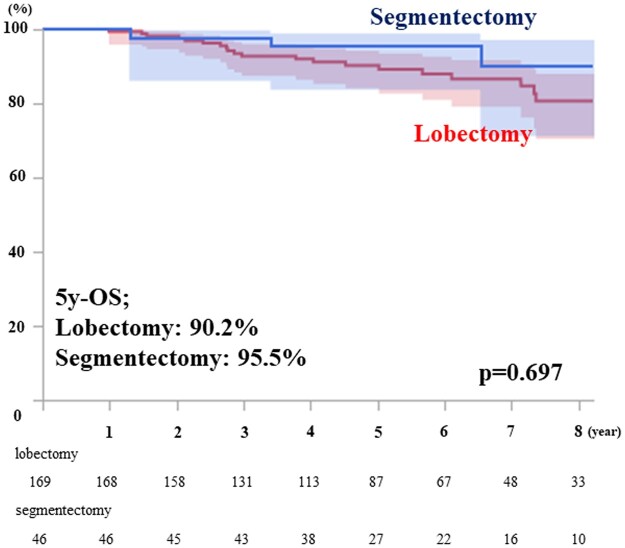
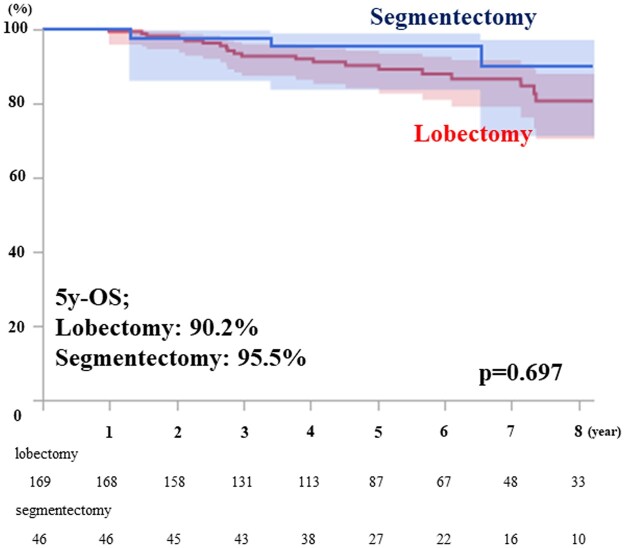
Results: Of the 215 eligible cases, segmentectomy and lobectomy were performed in 46 and 169 patients. Multivariable analysis revealed that standardized uptake value (hazard ratio: 1.148, 95% confidence interval: 1.032-1.276, P = 0.011) was an independently significant prognosticators of OS, while the operative mode was not associated (hazard ratio: 0.635, 95% confidence interval: 0.132-3.049, P = 0.570). The 5 y-OS was excellent and did not differ significantly between segmentectomy and lobectomy (95.5% vs 90.2%; P = 0.697), which was also shown in the propensity score analysis (96.8% vs 94.0%; P = 0.406), with a median follow-up time of 5.2 years. Locoregional recurrence was found in 2 (4.3%) segmentectomy and 13 (7.7%) lobectomy (P = 0.443). In the subgroup analysis stratified by solid component size, the 5 y-OS was similar between segmentectomy and lobectomy in the c-T1b and c-T1c groups, respectively [c-T1b (n = 163): 94.1% vs 91.8%; P = 0.887 and c-T1c (n = 52): 100% vs 84.9%; P = 0.197].
Conclusions: Segmentectomy showed similar oncological results compared to lobectomy in solid-predominant NSCLC with a ground-glass opacity component >2-3 cm in maximum tumour size. More prospective randomized trials are needed to adequately expand the indication of anatomic segmentectomy for early-stage NSCLC.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
