{"title":"A case of nail sarcoidosis with rich clinical findings.","authors":"Can Baykal, Zeynep Yılmaz, Tuğba Atcı","doi":"10.36141/svdld.v39i3.11525","DOIUrl":null,"url":null,"abstract":"To the editor, As skin lesions are observed in 10-35% of sarcoidosis patients, nail involvement is very rare which generally develops in the setting of chronic disease (14). Nail dystrophy is the most frequent nail change among several described findings (1,2,4-7). Herein, we report a case of sarcoidosis showing rich nail findings some of them rarely reported or not well-described. A 36-year-old man with pulmonary sarcoidosis (stage one) (Figure 1a,b) presented with multiple subcutaneous nodules on the face and extremities (Figure 2a). Histopathologic examination confirmed cutaneous sarcoidosis. Median splitting was noticed on one fingernail plate accompanied by a subungual reddish nodule and increased convexity on the proximal portion of the nail plate (Figure 2b). Magnetic resonance imaging of hand demonstrated soft tissue expansion at the location with increased convexity. In addition, bone cysts were detected in adjacent thumb and middle fingers radiologically (Figure 3a,b). Systemic methylprednisolone therapy resulted in significant improvement of the nail changes after four months of treatment (Figure 2c), along with the skin lesions that resolved completely. However, two months after cessation of the therapy, skin lesions recurred and distal notching associated with onycholysis and increased convexity of the nail plate appeared (Figure 2d). All lesions regressed after readministration of systemic corticosteroid (Figure 2e). Three years later, he was admitted with ulcerated plaques and subcutaneous nodules on arms (Figure 4a) and severe nail involvement (Figure 4b). Increased convexity, longitudinal ridging and subungual hyperkeratosis were observed on the previously affected third digit of the right hand (Figure 2f ), while a subungual reddish hyperkeratotic nodule on the thumbnail was detected which was associated with partial (median) nail plate loss (Figure 4c). Pitting, mild subungual hyperkeratosis, erythronychia and onycholysis were present on the third digit of the left hand (Figure 4d). Furthermore, total dystrophy (opaque, fragile, irregularly thickened nail plate) and subungual hyperkeratosis were observed on both big toenails accompanied by red-violaceous periungual discoloration (paronychial involvement) and tiny papules evaluated as lupus pernio of digit (Figure 4b,e). All lesions including periungual erythema, papules and nail findings regressed dramatically (Figure 4f ) after moderate-dose systemic corticosteroid. Letter to editor","PeriodicalId":21394,"journal":{"name":"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases","volume":"39 3","pages":"e2022032"},"PeriodicalIF":1.8000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/1e/0d/SVDLD-39-32.PMC9766855.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sarcoidosis, Vasculitis, and Diffuse Lung Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.36141/svdld.v39i3.11525","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 1
Abstract
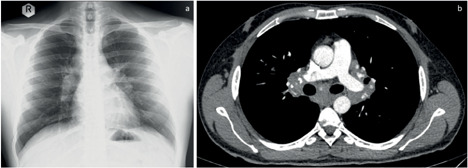
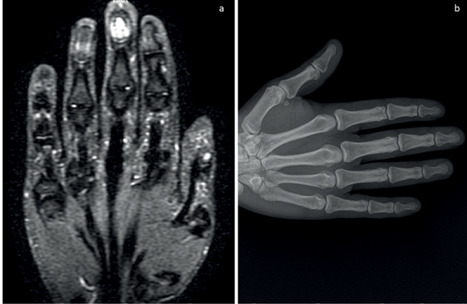
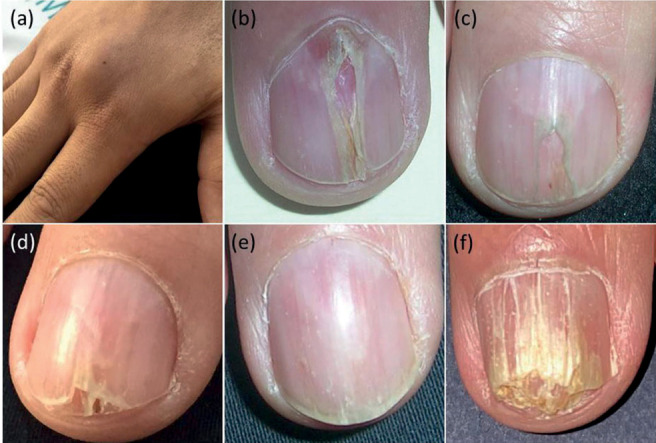
To the editor, As skin lesions are observed in 10-35% of sarcoidosis patients, nail involvement is very rare which generally develops in the setting of chronic disease (14). Nail dystrophy is the most frequent nail change among several described findings (1,2,4-7). Herein, we report a case of sarcoidosis showing rich nail findings some of them rarely reported or not well-described. A 36-year-old man with pulmonary sarcoidosis (stage one) (Figure 1a,b) presented with multiple subcutaneous nodules on the face and extremities (Figure 2a). Histopathologic examination confirmed cutaneous sarcoidosis. Median splitting was noticed on one fingernail plate accompanied by a subungual reddish nodule and increased convexity on the proximal portion of the nail plate (Figure 2b). Magnetic resonance imaging of hand demonstrated soft tissue expansion at the location with increased convexity. In addition, bone cysts were detected in adjacent thumb and middle fingers radiologically (Figure 3a,b). Systemic methylprednisolone therapy resulted in significant improvement of the nail changes after four months of treatment (Figure 2c), along with the skin lesions that resolved completely. However, two months after cessation of the therapy, skin lesions recurred and distal notching associated with onycholysis and increased convexity of the nail plate appeared (Figure 2d). All lesions regressed after readministration of systemic corticosteroid (Figure 2e). Three years later, he was admitted with ulcerated plaques and subcutaneous nodules on arms (Figure 4a) and severe nail involvement (Figure 4b). Increased convexity, longitudinal ridging and subungual hyperkeratosis were observed on the previously affected third digit of the right hand (Figure 2f ), while a subungual reddish hyperkeratotic nodule on the thumbnail was detected which was associated with partial (median) nail plate loss (Figure 4c). Pitting, mild subungual hyperkeratosis, erythronychia and onycholysis were present on the third digit of the left hand (Figure 4d). Furthermore, total dystrophy (opaque, fragile, irregularly thickened nail plate) and subungual hyperkeratosis were observed on both big toenails accompanied by red-violaceous periungual discoloration (paronychial involvement) and tiny papules evaluated as lupus pernio of digit (Figure 4b,e). All lesions including periungual erythema, papules and nail findings regressed dramatically (Figure 4f ) after moderate-dose systemic corticosteroid. Letter to editor
期刊介绍:
Sarcoidosis Vasculitis and Diffuse Lung Disease is a quarterly journal founded in 1984 by G. Rizzato. Now directed by R. Baughman (Cincinnati), P. Rottoli (Siena) and S. Tomassetti (Forlì), is the oldest and most prestigious Italian journal in such field.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
