Yasuyuki Shiraishi, Yuka Kurita, Miyuki Matsukawa, Hiromasa Mori
{"title":"Real-World Intravenous Diuretic Use to Treat Congestion in Patients With Heart Failure - An Observational Study Using a Research Database.","authors":"Yasuyuki Shiraishi, Yuka Kurita, Miyuki Matsukawa, Hiromasa Mori","doi":"10.1253/circrep.CR-22-0091","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Background:</i></b> Intravenous (IV) diuretics are key in the treatment of acute heart failure, but the time of administration can affect outcomes. Using a medical database, we assessed the real-world usage and clinical impact of IV diuretics after admission. <b><i>Methods and Results:</i></b> This observational study included hospitalized patients with heart failure who received IV diuretics. Relationships between IV diuretic use and clinical outcomes (duration of hospitalization, in-hospital mortality, readmission) were evaluated using analysis of variance or logistic regression. Overall, 9,653 patients (51.1% male) were assessed (mean age 80.9 years). Most (89.1%) patients had IV loop diuretic treatment initiated on Day 1 of hospitalization and 68.0% achieved the maximum dose on that day. The median duration of hospitalization was 17.0 days. In-hospital mortality was 9.2%; 13.7% of patients were readmitted within 3 months after discharge. There were prognostic relationships between IV diuretic usage and both duration of hospitalization and in-hospital mortality. On multivariable analysis, the time of maximum dose had the biggest impact on outcomes. Duration of hospitalization was prolonged and in-hospital mortality rates increased when the time of maximum dose was delayed. There was little correlation between IV diuretic use and readmission following discharge. <b><i>Conclusions:</i></b> Short-term outcomes (duration of hospitalization, in-hospital mortality) correlated with the time of maximum IV diuretic dose; thus, early initiation and subsequent modification of appropriate congestion treatment is critical for prognostic improvement.</p>","PeriodicalId":10276,"journal":{"name":"Circulation Reports","volume":"5 2","pages":"27-37"},"PeriodicalIF":0.0000,"publicationDate":"2023-02-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/af/cf/circrep-5-27.PMC9908529.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-22-0091","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
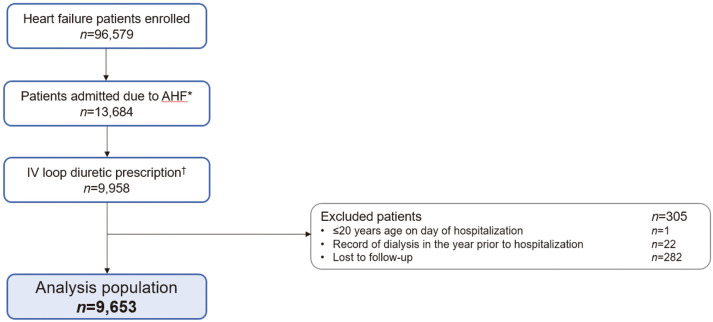
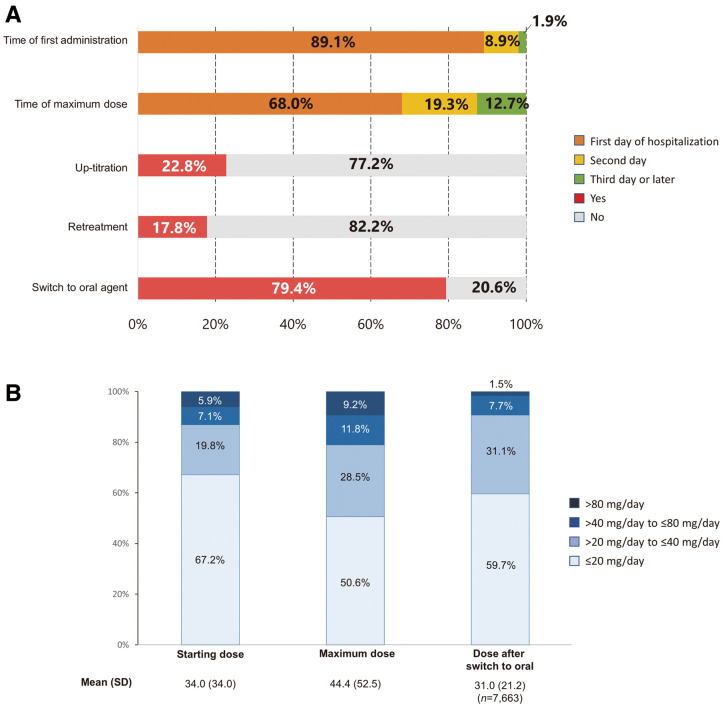
Background: Intravenous (IV) diuretics are key in the treatment of acute heart failure, but the time of administration can affect outcomes. Using a medical database, we assessed the real-world usage and clinical impact of IV diuretics after admission. Methods and Results: This observational study included hospitalized patients with heart failure who received IV diuretics. Relationships between IV diuretic use and clinical outcomes (duration of hospitalization, in-hospital mortality, readmission) were evaluated using analysis of variance or logistic regression. Overall, 9,653 patients (51.1% male) were assessed (mean age 80.9 years). Most (89.1%) patients had IV loop diuretic treatment initiated on Day 1 of hospitalization and 68.0% achieved the maximum dose on that day. The median duration of hospitalization was 17.0 days. In-hospital mortality was 9.2%; 13.7% of patients were readmitted within 3 months after discharge. There were prognostic relationships between IV diuretic usage and both duration of hospitalization and in-hospital mortality. On multivariable analysis, the time of maximum dose had the biggest impact on outcomes. Duration of hospitalization was prolonged and in-hospital mortality rates increased when the time of maximum dose was delayed. There was little correlation between IV diuretic use and readmission following discharge. Conclusions: Short-term outcomes (duration of hospitalization, in-hospital mortality) correlated with the time of maximum IV diuretic dose; thus, early initiation and subsequent modification of appropriate congestion treatment is critical for prognostic improvement.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
