Anwar A Alhulaibi, Abdulrahman M Alruwaili, Abdullah S Alotaibi, Fatima N Alshakhs, Habib S Alramadhan, Mohammed S Koudieh
{"title":"Validation of Various Prediction Scores for Cardiac Surgery-Associated Acute Kidney Injury.","authors":"Anwar A Alhulaibi, Abdulrahman M Alruwaili, Abdullah S Alotaibi, Fatima N Alshakhs, Habib S Alramadhan, Mohammed S Koudieh","doi":"10.37616/2212-5043.1322","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Following cardiac surgery, acute kidney injury (AKI) is a well-known complication that increases morbidity and mortality. This study was carried out to determine the factors associated with acute kidney injury and to assess the predictive value of three predictive scores for the development of AKI post-cardiac surgery in the Saudi community.</p><p><strong>Methods: </strong>In this retrospective study, the medical records of patients aged 18 years and above who underwent cardiac surgery on cardiopulmonary bypass (CPB) at Saud Albabtin Cardiac Center between January 2018 and March 2021 were reviewed. The first stage of both Kidney Disease Improving Global Outcomes (KDIGO) criteria and the risk, injury, failure, loss, end-stage (RIFLE) criteria were used to define AKI. The predicting value for acute kidney injury following cardiac surgery (AKICS score) and Renal replacement therapy for acute kidney injury (RRT-AKI) (Cleveland score, and SRI) were evaluated by area under receiver operating characteristic curve (AUROC) for the discrimination and Hosmer-Lemeshow test for the calibration.</p><p><strong>Results: </strong>Among the 329 patients evaluated, the total postoperative incidence of acute kidney injury was 26.4%. Moreover, the incidence of RRT-AKI was 2.1%. Using multivariate logistic analysis, the factors independently associated with AKI were CABG on pump-beating heart, presence of chronic kidney disease, pre-operative anemia, prolonged bypass time, and post-operative exposure to inotropes or vasopressors. For the prediction of CSA-AKI, the discrimination of AKICS (AUROC = 0.689) was poor, while the calibration (x2 = 9.380, P = 0.311) was fair. For RRT-AKI prediction, the discrimination of Cleveland score (AUROC = 0.717) was fair while the discrimination of SRI (AUROC = 0. 681) was poor. On the other hand, the calibration for both of them was fair (Cleveland score x2 = 3.339, P = 0.342; SRI x2 = 7.326, P = 0.120).</p><p><strong>Conclusion: </strong>In this single-center study, SRI score demonstrated a reasonably good prediction of RRT-AKI incidence. However, further researches are required to investigate the perioperative factors in order to create a unique risk score model that may be used in a population with widespread comorbidities.</p>","PeriodicalId":17319,"journal":{"name":"Journal of the Saudi Heart Association","volume":"34 4","pages":"222-231"},"PeriodicalIF":1.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a8/9e/sha222-231.PMC9930984.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Saudi Heart Association","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.37616/2212-5043.1322","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Background and objectives: Following cardiac surgery, acute kidney injury (AKI) is a well-known complication that increases morbidity and mortality. This study was carried out to determine the factors associated with acute kidney injury and to assess the predictive value of three predictive scores for the development of AKI post-cardiac surgery in the Saudi community.
Methods: In this retrospective study, the medical records of patients aged 18 years and above who underwent cardiac surgery on cardiopulmonary bypass (CPB) at Saud Albabtin Cardiac Center between January 2018 and March 2021 were reviewed. The first stage of both Kidney Disease Improving Global Outcomes (KDIGO) criteria and the risk, injury, failure, loss, end-stage (RIFLE) criteria were used to define AKI. The predicting value for acute kidney injury following cardiac surgery (AKICS score) and Renal replacement therapy for acute kidney injury (RRT-AKI) (Cleveland score, and SRI) were evaluated by area under receiver operating characteristic curve (AUROC) for the discrimination and Hosmer-Lemeshow test for the calibration.
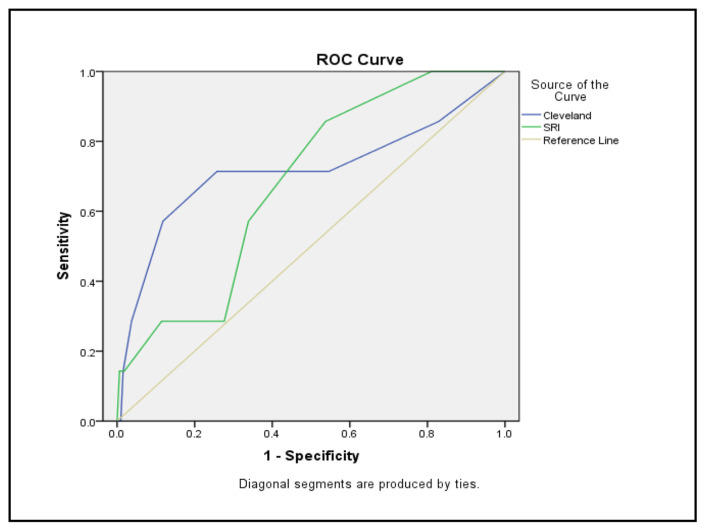
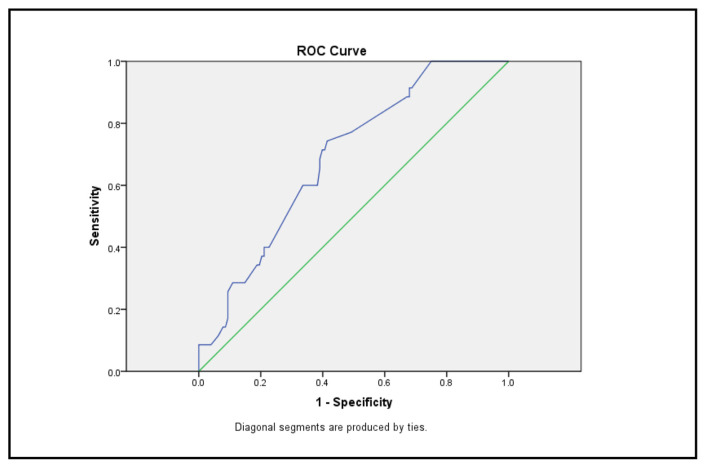
Results: Among the 329 patients evaluated, the total postoperative incidence of acute kidney injury was 26.4%. Moreover, the incidence of RRT-AKI was 2.1%. Using multivariate logistic analysis, the factors independently associated with AKI were CABG on pump-beating heart, presence of chronic kidney disease, pre-operative anemia, prolonged bypass time, and post-operative exposure to inotropes or vasopressors. For the prediction of CSA-AKI, the discrimination of AKICS (AUROC = 0.689) was poor, while the calibration (x2 = 9.380, P = 0.311) was fair. For RRT-AKI prediction, the discrimination of Cleveland score (AUROC = 0.717) was fair while the discrimination of SRI (AUROC = 0. 681) was poor. On the other hand, the calibration for both of them was fair (Cleveland score x2 = 3.339, P = 0.342; SRI x2 = 7.326, P = 0.120).
Conclusion: In this single-center study, SRI score demonstrated a reasonably good prediction of RRT-AKI incidence. However, further researches are required to investigate the perioperative factors in order to create a unique risk score model that may be used in a population with widespread comorbidities.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
