Jin Yu, Zhuo Shi, Jingjing Qian, Lianglong Ma, Baofu Zhang, Liyang Ying, Qiang Shu
{"title":"Analysis and comparison of failure causes of minimally invasive surgical closure of ventricular septal defects in children.","authors":"Jin Yu, Zhuo Shi, Jingjing Qian, Lianglong Ma, Baofu Zhang, Liyang Ying, Qiang Shu","doi":"10.1136/wjps-2022-000432","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The aims of the present study were to explore the causes of minimally invasive surgical ventricular septal defect (VSD) closure failure under transesophageal echocardiography guidance and thus to improve the success rate of surgical VSD closure.</p><p><strong>Methods: </strong>From January 2015 to December 2019, 522 children with VSD underwent minimally invasive surgical closure. Nineteen procedures (3.64%) were unsuccessful. The failure causes, VSD locations and surgical incision approaches were retrospectively analyzed.</p><p><strong>Results: </strong>Among the 19 patients (3.64%) with unsuccessful outcomes, 18 were switched to cardiopulmonary bypass (CPB) surgery, and 1 was closed successfully using an occlusion device a year later. The causes of failure included occlusion device shedding or shifting (n=6), failure of the guidewire (or the sheath) to pass through a small defect (n=5), device-related valve regurgitation (n=4), significant residual shunt (n=2), ventricular fibrillation (n=1), and continuous sharp blood pressure decreases (n=1). Patients with high VSD had a slightly higher failure rate than those with perimembranous VSD (p=0.049), and its key reason is the high proportion of occlusion device shedding or shifting (p=0.001). No significant difference in the failure rate was found between patients with different surgical incision approaches.</p><p><strong>Conclusions: </strong>Minimally invasive surgery has a high success rate for perimembranous VSDs. Occlusion device shedding or shifting is the most common cause of failure. The shedding or shifting risk of eccentric occlusion devices being used only for high VSDs is much greater than that of concentric occlusion devices being used for perimembranous VSDs, which increases the risk of conversion to CPB surgery for high VSDs.</p>","PeriodicalId":23823,"journal":{"name":"World Journal of Pediatric Surgery","volume":"6 1","pages":"e000432"},"PeriodicalIF":1.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3a/87/wjps-2022-000432.PMC9933489.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Pediatric Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/wjps-2022-000432","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: The aims of the present study were to explore the causes of minimally invasive surgical ventricular septal defect (VSD) closure failure under transesophageal echocardiography guidance and thus to improve the success rate of surgical VSD closure.
Methods: From January 2015 to December 2019, 522 children with VSD underwent minimally invasive surgical closure. Nineteen procedures (3.64%) were unsuccessful. The failure causes, VSD locations and surgical incision approaches were retrospectively analyzed.
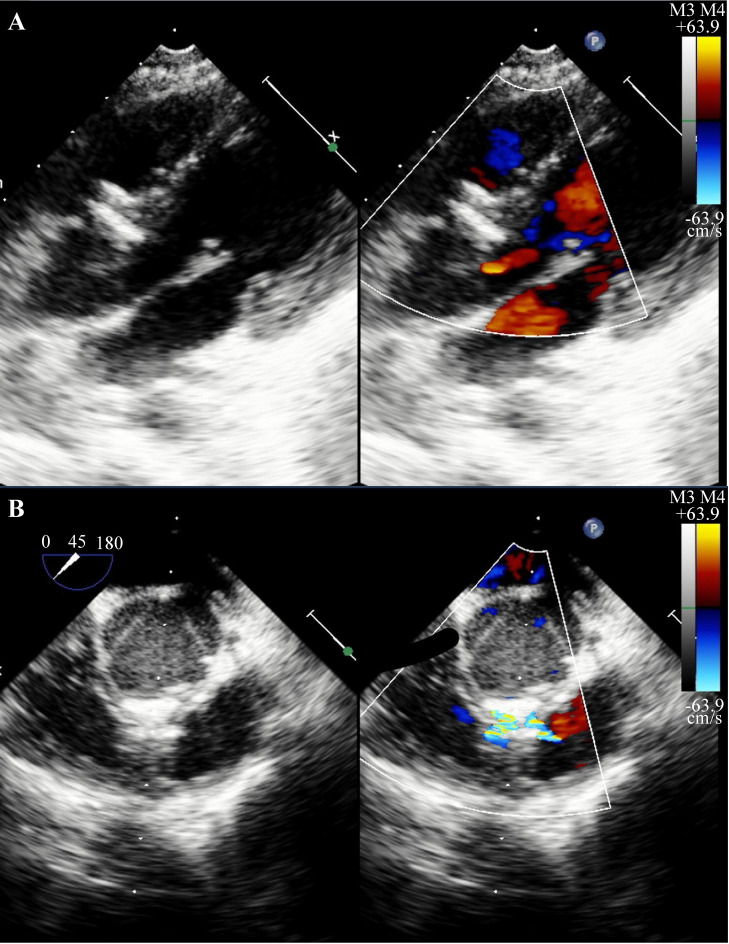
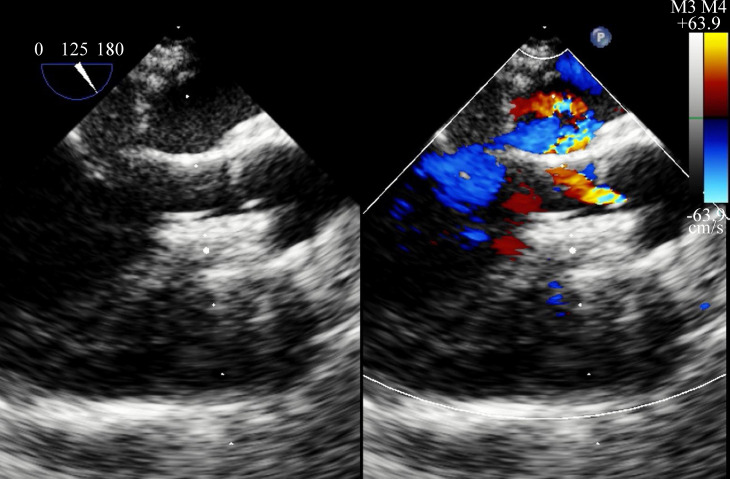
Results: Among the 19 patients (3.64%) with unsuccessful outcomes, 18 were switched to cardiopulmonary bypass (CPB) surgery, and 1 was closed successfully using an occlusion device a year later. The causes of failure included occlusion device shedding or shifting (n=6), failure of the guidewire (or the sheath) to pass through a small defect (n=5), device-related valve regurgitation (n=4), significant residual shunt (n=2), ventricular fibrillation (n=1), and continuous sharp blood pressure decreases (n=1). Patients with high VSD had a slightly higher failure rate than those with perimembranous VSD (p=0.049), and its key reason is the high proportion of occlusion device shedding or shifting (p=0.001). No significant difference in the failure rate was found between patients with different surgical incision approaches.
Conclusions: Minimally invasive surgery has a high success rate for perimembranous VSDs. Occlusion device shedding or shifting is the most common cause of failure. The shedding or shifting risk of eccentric occlusion devices being used only for high VSDs is much greater than that of concentric occlusion devices being used for perimembranous VSDs, which increases the risk of conversion to CPB surgery for high VSDs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
