Anna Politis, Hannah Cook, Hugo M L Cohen, Anne Pullyblank
{"title":"Improving the documentation of chaperones during intimate examinations in a surgical admissions unit: A four-stage approach.","authors":"Anna Politis, Hannah Cook, Hugo M L Cohen, Anne Pullyblank","doi":"10.3233/JRS-227031","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The General Medical Council (GMC) states that all intimate examinations should have a chaperone offered. Documentation of chaperone identity, or patient's refusal, is essential.</p><p><strong>Objective: </strong>This project aimed to improve documentation of chaperones during intimate examination of patients based in a Surgical Admissions Unit (SAU) within a large tertiary hospital in the Southwest of the UK.</p><p><strong>Methods: </strong>A Plan-Do-Study-Act (PDSA) cycle structure was used. Initial data collection and planning occurred in December 2019. Intervention implementation and analysis occurred from January 2020 to March 2021. Intervention 1 involved presenting results at a clinical governance meeting. Intervention 2 was information posters in the SAU and intervention 3 involved training sessions for nursing staff. Intervention 4 was editing the surgical clerking proforma.</p><p><strong>Results: </strong>Prior to interventions, chaperone identity or patient's refusal was correctly documented only 9.7% (N = 7 out of 72) of the time. Intervention 1 increased this to 34.6%. Following interventions 3 and 4, correct documentation was 25.0% and 28.6% respectively. After intervention 4 correct documentation was at 59.1%.</p><p><strong>Conclusions: </strong>Initial documentation of chaperones was poor. Interventions 1 to 3 were successful in educating clinicians how to document accurately, but engaging individuals in person was more successful than passive education through posters. Changing the proforma structure was the most successful intervention. This suggests a visual reminder for clinicians at the point of contact with the patient is the most effective way to encourage correct documentation of chaperones, improving patient care and clinical practice.</p>","PeriodicalId":45237,"journal":{"name":"INTERNATIONAL JOURNAL OF RISK & SAFETY IN MEDICINE","volume":"33 S1","pages":"S91-S95"},"PeriodicalIF":0.8000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/0b/e8/jrs-33-jrs227031.PMC9844066.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"INTERNATIONAL JOURNAL OF RISK & SAFETY IN MEDICINE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3233/JRS-227031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The General Medical Council (GMC) states that all intimate examinations should have a chaperone offered. Documentation of chaperone identity, or patient's refusal, is essential.
Objective: This project aimed to improve documentation of chaperones during intimate examination of patients based in a Surgical Admissions Unit (SAU) within a large tertiary hospital in the Southwest of the UK.
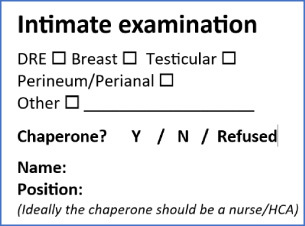
Methods: A Plan-Do-Study-Act (PDSA) cycle structure was used. Initial data collection and planning occurred in December 2019. Intervention implementation and analysis occurred from January 2020 to March 2021. Intervention 1 involved presenting results at a clinical governance meeting. Intervention 2 was information posters in the SAU and intervention 3 involved training sessions for nursing staff. Intervention 4 was editing the surgical clerking proforma.
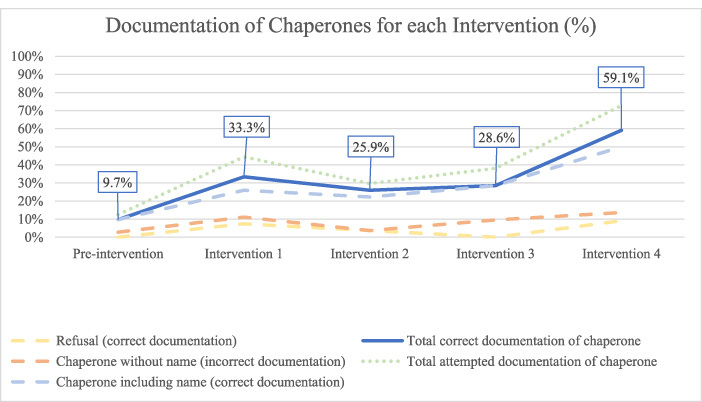
Results: Prior to interventions, chaperone identity or patient's refusal was correctly documented only 9.7% (N = 7 out of 72) of the time. Intervention 1 increased this to 34.6%. Following interventions 3 and 4, correct documentation was 25.0% and 28.6% respectively. After intervention 4 correct documentation was at 59.1%.
Conclusions: Initial documentation of chaperones was poor. Interventions 1 to 3 were successful in educating clinicians how to document accurately, but engaging individuals in person was more successful than passive education through posters. Changing the proforma structure was the most successful intervention. This suggests a visual reminder for clinicians at the point of contact with the patient is the most effective way to encourage correct documentation of chaperones, improving patient care and clinical practice.
期刊介绍:
The International Journal of Risk and Safety in Medicine is concerned with rendering the practice of medicine as safe as it can be; that involves promoting the highest possible quality of care, but also examining how those risks which are inevitable can be contained and managed. This is not exclusively a drugs journal. Recently it was decided to include in the subtitle of the journal three items to better indicate the scope of the journal, i.e. patient safety, pharmacovigilance and liability and the Editorial Board was adjusted accordingly. For each of these sections an Associate Editor was invited. We especially want to emphasize patient safety.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
