L Fabritz, D L Connolly, E Czarnecki, D Dudek, E Guasch, D Haase, T Huebner, A Zlahoda-Huzior, K Jolly, P Kirchhof, J Obergassel, U Schotten, E Vettorazzi, S J Winkelmann, A Zapf, R B Schnabel
{"title":"Smartphone and wearable detected atrial arrhythmias in Older Adults: Results of a fully digital European Case finding study.","authors":"L Fabritz, D L Connolly, E Czarnecki, D Dudek, E Guasch, D Haase, T Huebner, A Zlahoda-Huzior, K Jolly, P Kirchhof, J Obergassel, U Schotten, E Vettorazzi, S J Winkelmann, A Zapf, R B Schnabel","doi":"10.1093/ehjdh/ztac067","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Simplified detection of atrial arrhythmias via consumer-electronics would enable earlier therapy in at-risk populations. Whether this is feasible and effective in older populations is not known.</p><p><strong>Methods and results: </strong>The fully remote, investigator-initiated <b>Smart</b>phone and wearable detected atrial arrhythmia <b>in O</b>lder <b>A</b>dults <b>C</b>ase finding study (Smart in OAC-AFNET 9) digitally enrolled participants ≥65 years without known atrial fibrillation, not receiving oral anticoagulation in Germany, Poland, and Spain for 8 weeks. Participants were invited by media communications and direct contacts. Study procedures adhered to European data protection. Consenting participants received a wristband with a photoplethysmography sensor to be coupled to their smartphone. The primary outcome was the detection of atrial arrhythmias lasting 6 min or longer in the first 4 weeks of monitoring. Eight hundred and eighty-two older persons (age 71 ± 5 years, range 65-90, 500 (57%) women, 414 (47%) hypertension, and 97 (11%) diabetes) recorded signals. Most participants (72%) responded to adverts or word of mouth, leaflets (11%) or general practitioners (9%). Participation was completely remote in 469/882 persons (53%). During the first 4 weeks, participants transmitted PPG signals for 533/696 h (77% of the maximum possible time). Atrial arrhythmias were detected in 44 participants (5%) within 28 days, and in 53 (6%) within 8 weeks. Detection was highest in the first monitoring week [incidence rates: 1st week: 3.4% (95% confidence interval 2.4-4.9); 2nd-4th week: 0.55% (0.33-0.93)].</p><p><strong>Conclusion: </strong>Remote, digitally supported consumer-electronics-based screening is feasible in older European adults and identifies atrial arrhythmias in 5% of participants within 4 weeks of monitoring (NCT04579159).</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"3 4","pages":"610-625"},"PeriodicalIF":4.4000,"publicationDate":"2022-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9779806/pdf/","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztac067","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 7
Abstract
Aims: Simplified detection of atrial arrhythmias via consumer-electronics would enable earlier therapy in at-risk populations. Whether this is feasible and effective in older populations is not known.
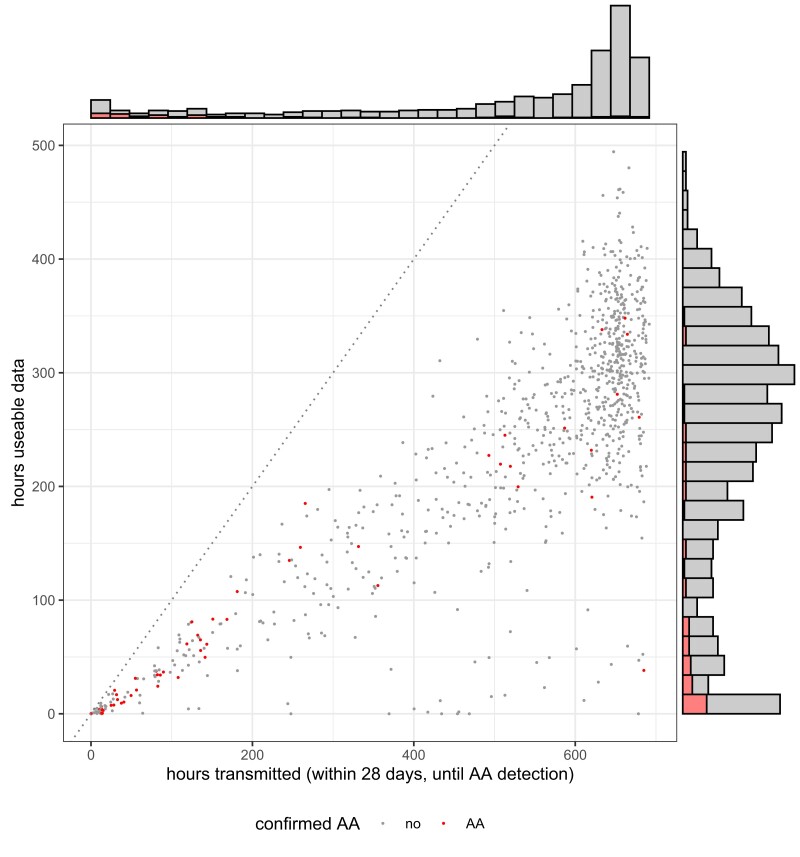
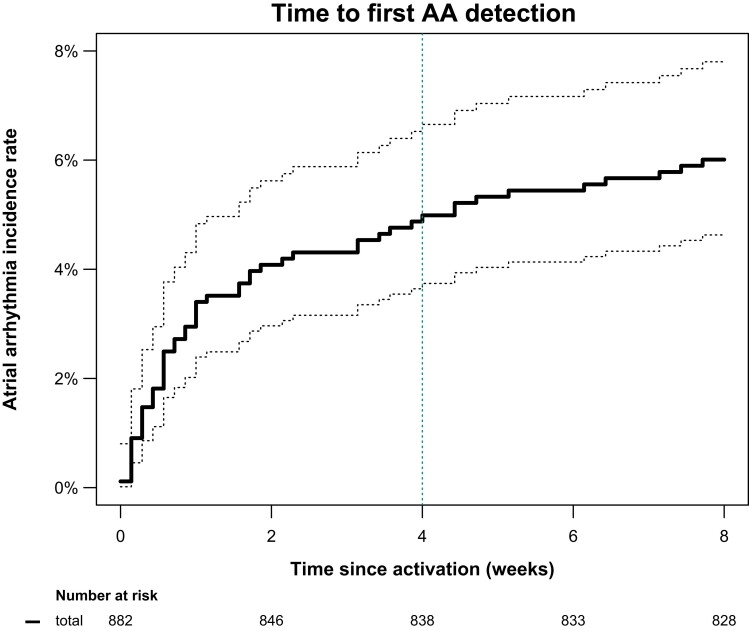
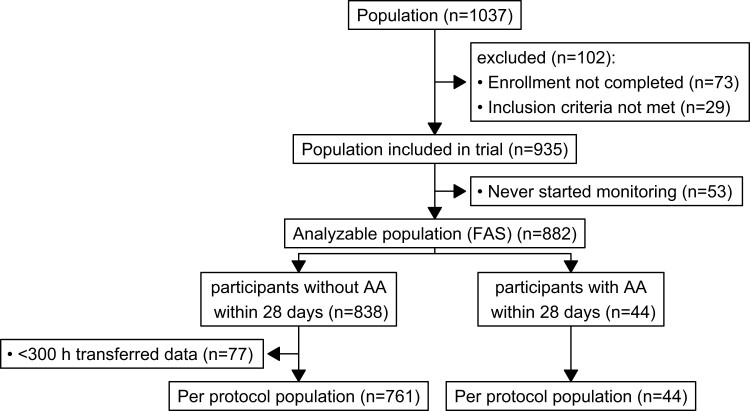
Methods and results: The fully remote, investigator-initiated Smartphone and wearable detected atrial arrhythmia in Older Adults Case finding study (Smart in OAC-AFNET 9) digitally enrolled participants ≥65 years without known atrial fibrillation, not receiving oral anticoagulation in Germany, Poland, and Spain for 8 weeks. Participants were invited by media communications and direct contacts. Study procedures adhered to European data protection. Consenting participants received a wristband with a photoplethysmography sensor to be coupled to their smartphone. The primary outcome was the detection of atrial arrhythmias lasting 6 min or longer in the first 4 weeks of monitoring. Eight hundred and eighty-two older persons (age 71 ± 5 years, range 65-90, 500 (57%) women, 414 (47%) hypertension, and 97 (11%) diabetes) recorded signals. Most participants (72%) responded to adverts or word of mouth, leaflets (11%) or general practitioners (9%). Participation was completely remote in 469/882 persons (53%). During the first 4 weeks, participants transmitted PPG signals for 533/696 h (77% of the maximum possible time). Atrial arrhythmias were detected in 44 participants (5%) within 28 days, and in 53 (6%) within 8 weeks. Detection was highest in the first monitoring week [incidence rates: 1st week: 3.4% (95% confidence interval 2.4-4.9); 2nd-4th week: 0.55% (0.33-0.93)].
Conclusion: Remote, digitally supported consumer-electronics-based screening is feasible in older European adults and identifies atrial arrhythmias in 5% of participants within 4 weeks of monitoring (NCT04579159).


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
