Soo Yung Kim, Sung Soo Kim, In Young Choi, Hyun Kuk Kim, Young Jae Ki, Dong Hyun Choi, Keun Ho Park
{"title":"Initial Experience with Left Bundle Branch Area Pacing in Patients with Atrioventricular Block and Impaired LV Function.","authors":"Soo Yung Kim, Sung Soo Kim, In Young Choi, Hyun Kuk Kim, Young Jae Ki, Dong Hyun Choi, Keun Ho Park","doi":"10.4068/cmj.2023.59.1.54","DOIUrl":null,"url":null,"abstract":"<p><p>Chronic right ventricular (RV) pacing can exacerbate heart failure in patients with a low left ventricular ejection fraction (LVEF). Left bundle branch area pacing (LBBAP) has emerged as a novel physiological pacing technique; however, information remains limited on its use among patients with a low EF. This study investigated the safety and short-term clinical outcomes of LBBAP among patients with impaired left ventricular (LV) function. This retrospective analysis of pacemakers at Chosun University Hospital, South Korea, included all patients with impaired LV function (EF<50%) who underwent pacemaker implantation for atrioventricular blockage from 2019-2022. Clinical characteristics, 12-lead electrocardiography findings, echocardiography findings, and laboratory parameters were evaluated. Composite outcomes were defined as all-cause mortality, cardiac death, and hospitalization due to heart failure during the 6-month follow-up. Altogether 57 patients (25 men; mean age, 77.4±10.8 y; LVEF, 41.5±3.8%) were divided into LBBAP (n=16), biventricular pacing (BVP; n=16), and conventional RV pacing (RVP; n=25) groups. In the LBBAP group, the mean paced QRS duration (pQRSd) was narrower (119.5±14.7 vs. 140.2±14.3 vs. 163.2±13.9; p<0.001) and cardiac troponin I level was elevated post-pacing (1.14±1.29 vs. 0.20±0.29 vs. 0.24±0.51, p=0.001). Lead parameters were stable. One patient was hospitalized, and four died (one patient each from heart failure admission, myocardial infarction, unexplained death, and pneumonia in RVP vs. one from intracerebral hemorrhage in BVP) during the follow-up period. In conclusion, LBBAP is feasible in patients with impaired LV function without acute or significant complications and provides a remarkably narrower pQRSd with a stable pacing threshold.</p>","PeriodicalId":10307,"journal":{"name":"Chonnam Medical Journal","volume":"59 1","pages":"54-60"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/98/d5/cmj-59-54.PMC9900220.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chonnam Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4068/cmj.2023.59.1.54","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
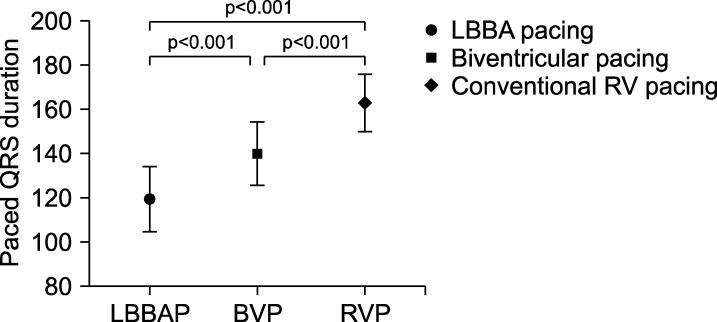
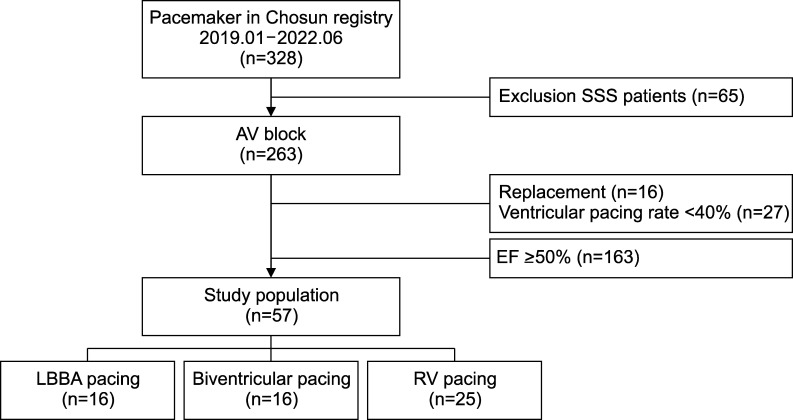
Chronic right ventricular (RV) pacing can exacerbate heart failure in patients with a low left ventricular ejection fraction (LVEF). Left bundle branch area pacing (LBBAP) has emerged as a novel physiological pacing technique; however, information remains limited on its use among patients with a low EF. This study investigated the safety and short-term clinical outcomes of LBBAP among patients with impaired left ventricular (LV) function. This retrospective analysis of pacemakers at Chosun University Hospital, South Korea, included all patients with impaired LV function (EF<50%) who underwent pacemaker implantation for atrioventricular blockage from 2019-2022. Clinical characteristics, 12-lead electrocardiography findings, echocardiography findings, and laboratory parameters were evaluated. Composite outcomes were defined as all-cause mortality, cardiac death, and hospitalization due to heart failure during the 6-month follow-up. Altogether 57 patients (25 men; mean age, 77.4±10.8 y; LVEF, 41.5±3.8%) were divided into LBBAP (n=16), biventricular pacing (BVP; n=16), and conventional RV pacing (RVP; n=25) groups. In the LBBAP group, the mean paced QRS duration (pQRSd) was narrower (119.5±14.7 vs. 140.2±14.3 vs. 163.2±13.9; p<0.001) and cardiac troponin I level was elevated post-pacing (1.14±1.29 vs. 0.20±0.29 vs. 0.24±0.51, p=0.001). Lead parameters were stable. One patient was hospitalized, and four died (one patient each from heart failure admission, myocardial infarction, unexplained death, and pneumonia in RVP vs. one from intracerebral hemorrhage in BVP) during the follow-up period. In conclusion, LBBAP is feasible in patients with impaired LV function without acute or significant complications and provides a remarkably narrower pQRSd with a stable pacing threshold.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
