Justin A Cline, Lisa M Frantz, Jessica M Adams, Bernard F Hearon
{"title":"Experience With Proximal Median Nerve Entrapment by the Lacertus Fibrosus.","authors":"Justin A Cline, Lisa M Frantz, Jessica M Adams, Bernard F Hearon","doi":"10.1177/15589447231153233","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unconscious bias of the clinician favors the diagnosis of carpal tunnel syndrome (CTS) in patients with median paresthesia. We hypothesized that more patients in this cohort would be diagnosed with proximal median nerve entrapment (PMNE) by strengthening our cognitive awareness of this alternative diagnosis. We also hypothesized that patients with PMNE may be successfully treated with surgical release of the lacertus fibrosus (LF).</p><p><strong>Methods: </strong>In this retrospective study, cases of median nerve decompression at the carpal tunnel and in the proximal forearm for the 2-year periods before and after adopting strategies to mitigate cognitive bias for CTS were enumerated. Patients diagnosed with PMNE and treated by LF release under local anesthesia were evaluated to determine surgical outcome at minimum 2-year follow-up. Primary outcome measures were changes in preoperative median paresthesia and proximal median-innervated muscle strength.</p><p><strong>Results: </strong>There was a statistically significant increase in PMNE cases identified after our heightened surveillance was initiated (<i>z</i> = 3.433, <i>P</i> < .001). In 10 of 12 cases, the patient had previous ipsilateral open carpal tunnel release (CTR) but experienced recurrent median paresthesia. In 8 cases evaluated an average of 5 years after LF release, there was improvement in median paresthesia and resolution of median-innervated muscle weakness.</p><p><strong>Conclusions: </strong>Owing to cognitive bias, some patients with PMNE may be misdiagnosed with CTS. All patients with median paresthesia, particularly those with persistent or recurrent symptoms after CTR, should be assessed for PMNE. Surgical release limited to the LF may be an effective treatment for PMNE.</p>","PeriodicalId":12902,"journal":{"name":"HAND","volume":" ","pages":"904-911"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11342709/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"HAND","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/15589447231153233","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/3/1 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Unconscious bias of the clinician favors the diagnosis of carpal tunnel syndrome (CTS) in patients with median paresthesia. We hypothesized that more patients in this cohort would be diagnosed with proximal median nerve entrapment (PMNE) by strengthening our cognitive awareness of this alternative diagnosis. We also hypothesized that patients with PMNE may be successfully treated with surgical release of the lacertus fibrosus (LF).
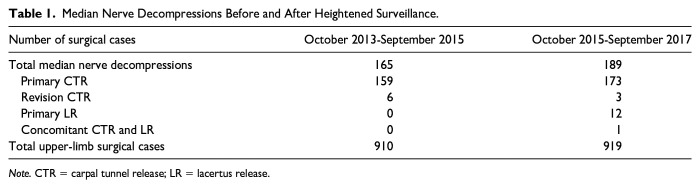
Methods: In this retrospective study, cases of median nerve decompression at the carpal tunnel and in the proximal forearm for the 2-year periods before and after adopting strategies to mitigate cognitive bias for CTS were enumerated. Patients diagnosed with PMNE and treated by LF release under local anesthesia were evaluated to determine surgical outcome at minimum 2-year follow-up. Primary outcome measures were changes in preoperative median paresthesia and proximal median-innervated muscle strength.
Results: There was a statistically significant increase in PMNE cases identified after our heightened surveillance was initiated (z = 3.433, P < .001). In 10 of 12 cases, the patient had previous ipsilateral open carpal tunnel release (CTR) but experienced recurrent median paresthesia. In 8 cases evaluated an average of 5 years after LF release, there was improvement in median paresthesia and resolution of median-innervated muscle weakness.
Conclusions: Owing to cognitive bias, some patients with PMNE may be misdiagnosed with CTS. All patients with median paresthesia, particularly those with persistent or recurrent symptoms after CTR, should be assessed for PMNE. Surgical release limited to the LF may be an effective treatment for PMNE.
期刊介绍:
HAND is the official journal of the American Association for Hand Surgery and is a peer-reviewed journal featuring articles written by clinicians worldwide presenting current research and clinical work in the field of hand surgery. It features articles related to all aspects of hand and upper extremity surgery and the post operative care and rehabilitation of the hand.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
