{"title":"Dyspnea in Oncological Patients: a Brain Teaser.","authors":"Kalliopi Keramida, Athanasios Kostoulas","doi":"10.15420/ecr.2021.62","DOIUrl":null,"url":null,"abstract":"<p><p>Dyspnea is one of the most common symptoms in oncological patients with greater prevalence in lung cancer and advanced disease states. Causes of dyspnea can be directly or indirectly associated with cancer, anti-neoplastic therapies and comorbidities unrelated to cancer. Routine screening of dyspnea is suggested for all oncological patients by using unidimensional, simple scales and multidimensional tools to capture more domains affected by this symptom and to assess the effectiveness of interventions. The first step in the treatment algorithm of dyspnea is the identification of potentially reversible causes; if no specific cause is depicted, symptomatic treatment with non-pharmacological and pharmacological interventions is suggested. Referral to palliative care and continuous palliative sedation are the last resort in patients with a very limited life expectancy of not more than a few days for symptomatic relief and to decrease of the distress of patients and caregivers.</p>","PeriodicalId":45957,"journal":{"name":"European Cardiology Review","volume":"18 ","pages":"e03"},"PeriodicalIF":3.6000,"publicationDate":"2023-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/cc/f3/ecr-18-e03.PMC9947930.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Cardiology Review","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15420/ecr.2021.62","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
Abstract
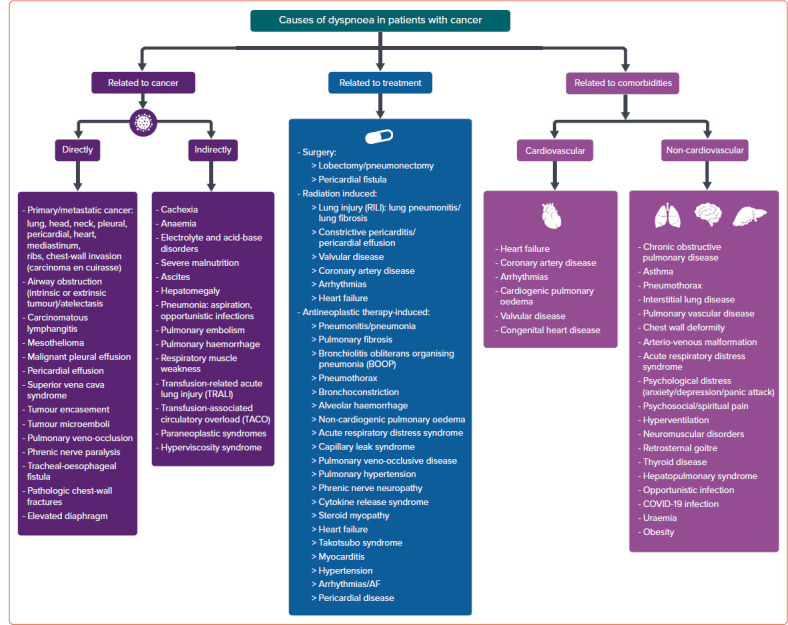
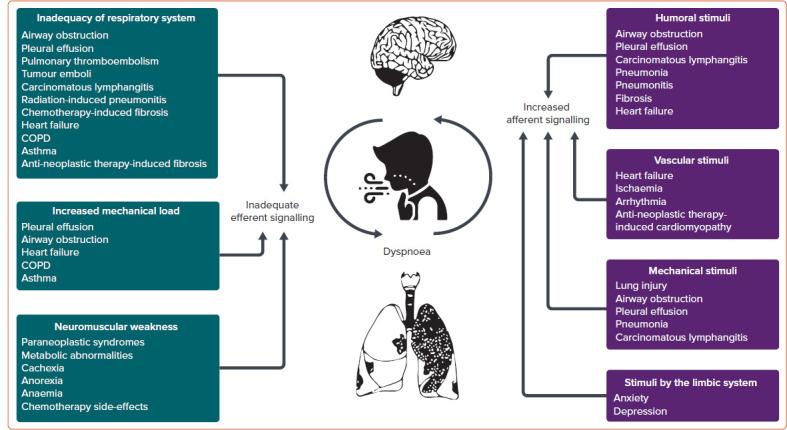
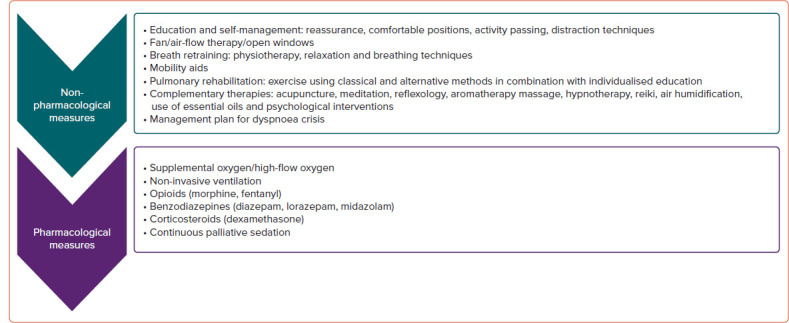
Dyspnea is one of the most common symptoms in oncological patients with greater prevalence in lung cancer and advanced disease states. Causes of dyspnea can be directly or indirectly associated with cancer, anti-neoplastic therapies and comorbidities unrelated to cancer. Routine screening of dyspnea is suggested for all oncological patients by using unidimensional, simple scales and multidimensional tools to capture more domains affected by this symptom and to assess the effectiveness of interventions. The first step in the treatment algorithm of dyspnea is the identification of potentially reversible causes; if no specific cause is depicted, symptomatic treatment with non-pharmacological and pharmacological interventions is suggested. Referral to palliative care and continuous palliative sedation are the last resort in patients with a very limited life expectancy of not more than a few days for symptomatic relief and to decrease of the distress of patients and caregivers.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
