{"title":"The parieto-occipital groove is a fissure, not a sulcus: Relevance to prenatal ultrasonographic imaging","authors":"Harvey B. Sarnat, Ian Suchet","doi":"10.1002/cns3.20044","DOIUrl":null,"url":null,"abstract":"<p>Both fissures and sulci are permanent indentations, grooves, or foldings of the cerebral cortex. They are distinguished in large part by timing: fissures form in the first half of gestation and sulci in the second half. A notable exception is the <i>sulcus limitans</i>, a shallow longitudinal groove in the horizontal axis of the embryonic neural tube that extends throughout the spinal cord and brainstem to the mesencephalon and rostrally into the wall of the third ventricle. It is most evident in the lateral wall of the fetal spinal central canal, cerebral aqueduct, and third ventricle and demarcates alar and basal plates of primordial gray matter to denote the separation of dorsal and ventral horns in the spinal cord and sensory and motor cranial nuclei in the brainstem. Other small embryonic grooves, such as the one that demarcates the lateral from the medial ganglionic eminences, also were called <i>sulci</i>, having been named from antiquity to the late 19th century. All sulci in the embryonic brain are transitory, unlike the permanent sulci of the cerebral cortex or interfolial sulci of the cerebellar cortex.</p><p>The earliest true fissure to form is the <i>interhemispheric fissure</i>, secondary to cleavage of the prosencephalon at four to five weeks' gestational age (GA); the last fissure to form is the <i>lateral cerebral (sylvian) fissure</i> because of bending of the <i>telencephalic flexure</i>, the primitive telencephalic hemisphere in which the caudal end of the early telencephalon becomes not the occipital pole but rather the rostral pole of the temporal lobe.<span><sup>1</sup></span> Examples of intermediately timed fissures are the hippocampal and calcarine. Another distinction is that fissures result mainly from external mechanical or physical forces, whereas sulci principally form because of intrinsic growth.<span><sup>1</sup></span> Convolutions are needed so that the cerebrum at term and the fetal head at birth are not so large as to pose an intrapartum traumatic risk to both fetus and mother, which also would be conducive to survival of the species. Small mammals, such as rodents and lagomorphs, have smooth nonconvoluted brains even at maturity because the number of cortical neurons is not enough to require folding; an interhemispheric fissure forms in mice, rats, squirrels, and rabbits, but a lateral cerebral fissure does not develop.<span><sup>2</sup></span> In humans and other large mammals, the sequence of gyral and sulcal formation follows a time-linked predictable program leading to precise gyral identification at each gestational age of the late second and third trimesters and in the mature brain.<span><sup>3</sup></span> Cortical sulcation not only enables a larger surface area without a concomitant increase in cerebral volume but also provides for intracerebral connectivity conducive to more complex synaptic circuitry.<span><sup>4</sup></span></p><p>The development of fissures and sulci often is altered in many malformations of the human embryonic and fetal brain. In alobar holoprosencephaly, neither the interhemispheric fissure nor the lateral cerebral (sylvian) fissure develop and gyration is absent or abnormal.<span><sup>2, 5, 6</sup></span> In lissencephaly/pachygyria the fissures are formed but convolutions are absent or poorly formed.<span><sup>2</sup></span> Other examples of abnormal sulcation include polymicrogyria, schizencephaly,<span><sup>2</sup></span> and “simplification” of the gyral pattern with microcephaly.<span><sup>7</sup></span></p><p>The normal parieto-occipital groove is variably called in both neuroanatomical textbooks and numerous peer-reviewed articles a fissure in some<span><sup>3, 8, 9</sup></span> and a sulcus in others.<span><sup>10-12</sup></span> If it is a fissure, it is the last fissure to appear and if a sulcus, the first sulcus to be formed. Perhaps the lateral cerebral could still retain its status as the last to form because technically the operculum is not yet the sylvian fissure until it closes late in the third trimester. <i>Because the parieto-occipital groove separates two major lobes of the cortex and because it becomes evident in the first half of gestation, at 16 weeks, we prefer to consider it a fissure</i>. Separation between lobes is not an absolute criterion, however. The lateral cerebral (sylvian) fissure separates the frontal and temporal lobes, but the much later forming central sulcus demarcates the frontal from the parietal lobe. The calcarine fissure is entirely within the medial surface of the occipital lobe.</p><p>The parieto-occipital fissure is an important and practical prenatal landmark of cerebral cortical maturation reliably detected by ultrasonic imaging (Figure 1A–F) from 16 weeks' gestation or by fetal magnetic resonance imaging, at times confirmed neuropathologically even earlier than by imaging. In an axial plane it is best visualized near the upper margin of the occipital horns of the lateral ventricles. It also can be visualized in a parasagittal plane through the medial surface of the posterior half of the cerebral hemisphere, almost perpendicular to the calcarine fissure (Figure 1G). It is first seen sonographically in the axial plane as a small dot on the cortical surface at 16 weeks' GA; is identified in 50% of fetuses at 18 weeks' GA and 93.3% of fetuses at 19 weeks' GA; and is always visible after 20 weeks' GA.<span><sup>13</sup></span> Its depth may be measured from the midline by drawing a perpendicular line extending from the apex of the fissure. This parieto-occipital fissure is longer and deeper than most of the sulci that form at the cortical surface during gyration in the second half of gestation, except perhaps for the long central sulcus in the vertical axis that demarcates the frontal and parietal lobes. Depth tables of the parieto-occipital fissure are reported from 18 to 32 weeks' GA.<span><sup>14</sup></span> Ultrasonic imaging is now a primary technique of obstetricians and perinatologists to assess cerebral development and its disorders and is used routinely. Pediatric neurologists who consult prenatally need to become more familiar with ultrasonic imaging.</p><p>Increasing precision of prenatal neuroimaging and its interpretation by perinatologists is resulting in increasing consultation requests to pediatric neurologists, and especially to those dedicated to neuro-intensive care, for abnormal fetal findings. It is imperative that pediatric neurologists become familiar with advances in maternal-fetal medicine and be prepared for prenatal diagnoses. Standardization of terminology enhances comprehension and communication in both the basic and clinical neurosciences.<span><sup>15</sup></span> Semantics do matter!</p><p><b>Harvey B. Sarnat</b>: Conceptualization; Writing—original draft; Writing—review & editing. <b>Ian Suchet</b>: Conceptualization; Data curation; Visualization; Writing—review & editing.</p><p>Harvey B. Sarnat serves on the editorial board of <i>Annals of the Child Neurology Society</i>. Ian Suchet has no conflict of interest to declare. The authors have no financial disclosures.</p>","PeriodicalId":72232,"journal":{"name":"Annals of the Child Neurology Society","volume":"1 4","pages":"269-272"},"PeriodicalIF":0.0000,"publicationDate":"2023-10-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/cns3.20044","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of the Child Neurology Society","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cns3.20044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Both fissures and sulci are permanent indentations, grooves, or foldings of the cerebral cortex. They are distinguished in large part by timing: fissures form in the first half of gestation and sulci in the second half. A notable exception is the sulcus limitans, a shallow longitudinal groove in the horizontal axis of the embryonic neural tube that extends throughout the spinal cord and brainstem to the mesencephalon and rostrally into the wall of the third ventricle. It is most evident in the lateral wall of the fetal spinal central canal, cerebral aqueduct, and third ventricle and demarcates alar and basal plates of primordial gray matter to denote the separation of dorsal and ventral horns in the spinal cord and sensory and motor cranial nuclei in the brainstem. Other small embryonic grooves, such as the one that demarcates the lateral from the medial ganglionic eminences, also were called sulci, having been named from antiquity to the late 19th century. All sulci in the embryonic brain are transitory, unlike the permanent sulci of the cerebral cortex or interfolial sulci of the cerebellar cortex.
The earliest true fissure to form is the interhemispheric fissure, secondary to cleavage of the prosencephalon at four to five weeks' gestational age (GA); the last fissure to form is the lateral cerebral (sylvian) fissure because of bending of the telencephalic flexure, the primitive telencephalic hemisphere in which the caudal end of the early telencephalon becomes not the occipital pole but rather the rostral pole of the temporal lobe.1 Examples of intermediately timed fissures are the hippocampal and calcarine. Another distinction is that fissures result mainly from external mechanical or physical forces, whereas sulci principally form because of intrinsic growth.1 Convolutions are needed so that the cerebrum at term and the fetal head at birth are not so large as to pose an intrapartum traumatic risk to both fetus and mother, which also would be conducive to survival of the species. Small mammals, such as rodents and lagomorphs, have smooth nonconvoluted brains even at maturity because the number of cortical neurons is not enough to require folding; an interhemispheric fissure forms in mice, rats, squirrels, and rabbits, but a lateral cerebral fissure does not develop.2 In humans and other large mammals, the sequence of gyral and sulcal formation follows a time-linked predictable program leading to precise gyral identification at each gestational age of the late second and third trimesters and in the mature brain.3 Cortical sulcation not only enables a larger surface area without a concomitant increase in cerebral volume but also provides for intracerebral connectivity conducive to more complex synaptic circuitry.4
The development of fissures and sulci often is altered in many malformations of the human embryonic and fetal brain. In alobar holoprosencephaly, neither the interhemispheric fissure nor the lateral cerebral (sylvian) fissure develop and gyration is absent or abnormal.2, 5, 6 In lissencephaly/pachygyria the fissures are formed but convolutions are absent or poorly formed.2 Other examples of abnormal sulcation include polymicrogyria, schizencephaly,2 and “simplification” of the gyral pattern with microcephaly.7
The normal parieto-occipital groove is variably called in both neuroanatomical textbooks and numerous peer-reviewed articles a fissure in some3, 8, 9 and a sulcus in others.10-12 If it is a fissure, it is the last fissure to appear and if a sulcus, the first sulcus to be formed. Perhaps the lateral cerebral could still retain its status as the last to form because technically the operculum is not yet the sylvian fissure until it closes late in the third trimester. Because the parieto-occipital groove separates two major lobes of the cortex and because it becomes evident in the first half of gestation, at 16 weeks, we prefer to consider it a fissure. Separation between lobes is not an absolute criterion, however. The lateral cerebral (sylvian) fissure separates the frontal and temporal lobes, but the much later forming central sulcus demarcates the frontal from the parietal lobe. The calcarine fissure is entirely within the medial surface of the occipital lobe.
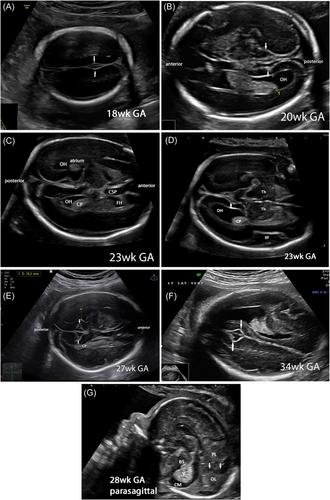
The parieto-occipital fissure is an important and practical prenatal landmark of cerebral cortical maturation reliably detected by ultrasonic imaging (Figure 1A–F) from 16 weeks' gestation or by fetal magnetic resonance imaging, at times confirmed neuropathologically even earlier than by imaging. In an axial plane it is best visualized near the upper margin of the occipital horns of the lateral ventricles. It also can be visualized in a parasagittal plane through the medial surface of the posterior half of the cerebral hemisphere, almost perpendicular to the calcarine fissure (Figure 1G). It is first seen sonographically in the axial plane as a small dot on the cortical surface at 16 weeks' GA; is identified in 50% of fetuses at 18 weeks' GA and 93.3% of fetuses at 19 weeks' GA; and is always visible after 20 weeks' GA.13 Its depth may be measured from the midline by drawing a perpendicular line extending from the apex of the fissure. This parieto-occipital fissure is longer and deeper than most of the sulci that form at the cortical surface during gyration in the second half of gestation, except perhaps for the long central sulcus in the vertical axis that demarcates the frontal and parietal lobes. Depth tables of the parieto-occipital fissure are reported from 18 to 32 weeks' GA.14 Ultrasonic imaging is now a primary technique of obstetricians and perinatologists to assess cerebral development and its disorders and is used routinely. Pediatric neurologists who consult prenatally need to become more familiar with ultrasonic imaging.
Increasing precision of prenatal neuroimaging and its interpretation by perinatologists is resulting in increasing consultation requests to pediatric neurologists, and especially to those dedicated to neuro-intensive care, for abnormal fetal findings. It is imperative that pediatric neurologists become familiar with advances in maternal-fetal medicine and be prepared for prenatal diagnoses. Standardization of terminology enhances comprehension and communication in both the basic and clinical neurosciences.15 Semantics do matter!
Harvey B. Sarnat: Conceptualization; Writing—original draft; Writing—review & editing. Ian Suchet: Conceptualization; Data curation; Visualization; Writing—review & editing.
Harvey B. Sarnat serves on the editorial board of Annals of the Child Neurology Society. Ian Suchet has no conflict of interest to declare. The authors have no financial disclosures.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
